
INTRODUCTION
Every so often, the world of restorative dentistry changes markedly, and 2019 will go down in dental history as a year of revolution rather than evolution in composite technology. This includes new formulations of bonding agents (the tenth generation?) as well as advanced formulas and adaptive capabilities of composites. Our arsenal of products that mimic tooth structure has increased and now includes bonding agents that can bond to any tooth and, for the first time, a material that can match virtually any tooth color using only one shade of composite!
Composite Dentistry Historical Breakthroughs
A brief history of composite restorations begins in the middle of the 20th Century. Dr. Michael Buonocore discovered that phosphoric acid can increase mechanical bonding to tooth structure in 1955.1 RL Bowen is credited with the invention of dental composites in 1962.2
 |
 |
| Figures 1 and 2. Many dentists still remember Concise composite resin (3M), one of the first macrofill composites. Henry Schein used a similar formula for its “Composite” material. |
 |
| Figure 3. ACTIVA BioACTIVE RESTORATIVE (Pulpdent) is one of the first bioactive composites. Produced in restorative, cement, and base consistencies, this family of products allows fluid and mineral transport between the material and the tooth throughout the lifetime of the restoration. |
In the 1970s, the first commercially successful restorative composite resins (Concise [3M] and Adaptic [Dentsply Sirona]) were introduced. They were considered macrofills, containing very large filler particles and measuring zero to 5 μm. The irregular-edged, large particle size made them very difficult to polish even though they were rather strong. The formula for Concise is still sold in the United States under the Henry Schein label, and, curiously, it is named Composite (Figures 1 and 2).
In the 1980s, microfill composites made their debut, including Durafill VS (Kulzer) and Renamel (Cosmedent).3 They continue to have properties that are virtually the opposite of the macrofills: excellent polishability and aesthetics. However, most did not exhibit the strength required for use in occlusal load-bearing areas, with one notable exception: a microfill formulated for posterior teeth called Heliomolar (and later Heliomolar HB) (Ivoclar Vivadent).
During the 1990s, hybrids and the layering of composites became popular. The earliest hybrids were not easily polishable.4 Subsequent products (such as the original Esthet-X [Dentsply Sirona]) were stronger, but their aesthetics did not match today’s composite resin options.
The 2000s brought multiple new formulations along with better aesthetics. Translucent and opaque shades have allowed us to truly mimic tooth structure for the first time. In fact, many of today’s products create a need to buy kits that contain upwards of 30 shades. This has created problems for offices that needed to stock all of these shades; namely, that many of the shades would not be used during the product life span. In addition, as this millennium arrived, nanofilled composites were introduced. These consisted of nano particles (5 to 75 nm) and nanocluster fillers. They include particles from 5 to 20 nm in size.4,5 A smoother finish and shine resulted as well as stronger restorations.6 These products include Tetric EvoCeram (Ivoclar Vivadent) and Filtek Supreme Plus (3M).
 |
 |
| Figure 4. Tokuyama Universal Bond (Tokuyama Dental America) is a next-generation bonding agent that bonds to all tooth surfaces and dental materials and does not require light activation. |
Figure 5. Omnichroma (Tokuyama Dental America) is a next-generation composite material with fillers that changes the way light is transmitted. This allows a single shade of the material to match virtually every tooth. |
Bulk-fill composites have become accepted by a larger population of dentists in the 2010s. Companies have promoted less polymerization shrinkage and a higher depth of cure up to 4.0 mm.7 The first highly accepted flowable bulk fill, SureFil SDR flow (Dentsply Sirona), was limited to use as a base under restorations.7 Newer flowable bulk-fill agents, including Tetric EvoCeram Bulk Fill (Ivoclar Vivadent) and Estelite Bulk Fill Flow (Tokuyama Dental America), require no capping layer of another composite. They show higher strength and aesthetics; however, some bulk fills can be more translucent. This can be a positive or negative attribute, depending on the situation.
Evolutionary Changes
Bioactive and bioceramic products have made inroads during this past decade. The ACTIVA BioACTIVE RESTORATIVE (Pulpdent) line of products (Figure 3), TheraCal LC (BISCO Dental Products) cavity liner, and Ceramir (Doxa Dental) cement exhibit positive properties that stand to benefit diverse groups, if not all dental patients. The essence of bioactivity is the ability to continue to be reactive during the entire product lifetime as opposed to an inert material that fills a space but does not continue as an active material. Fluoride release and the active transport of minerals and water may increase the longevity of these restorations, repair damaged tooth structure, and help them to stem decay.8
In 2007, Tokuyama Dental America introduced the first 100% supra-nano spherical filled resin composite called Estelite Sigma Quick. This is a universal composite that allows for high polishability due to the spherically designed particles that are manufactured without irregular edges. This concept also led to the development of the acclaimed premium polychromatic composite, Estelite Omega (Tokuyama Dental America).
In 2018, we have witnessed the launch of other spherical-particle-based composites, notably Harmonize (KaVo Kerr) and Brilliant Everglow (COLTENE). Brilliant Everglow is termed an “all-round” material with dual shade compules, whereas Harmonize relies on “crosslinks of spherical silica and zirconia particles together with positive and negative charges.”
Revolutionary Change
This year, 2019, marks the introduction of several products that will buck the trends of the last 20 years in restorative dentistry. The first, Tokuyama Universal B
ond (Tokuyama Dental America) (Figure 4), is a truly universal agent that bonds to virtually everything. This includes direct, indirect, light-cure, self-cure, and dual-cure materials in self-etch, total-etch, and selective-etch modes. What makes this material a paradigm shifter is that no light curing, primers, or activators are needed. The clinician mixes equal parts A and B, applies it to dentin and enamel, and air dries it to polymerize the bonding agent prior to adding the composite of choice. Many dentists have not used a bonding agent without light curing since the early days of Tenure (DenMat) about 20 years ago.
Also, 2019 brings the introduction of another truly groundbreaking material, Omnichroma (Tokuyama Dental America) (Figure 5). This is the first omnichromatic composite resin-based material that will match any tooth, any shade, on any patient. In an era when many composite materials require having multiple shades available for use in any given clinical situation, Omnichroma poses a unique opportunity for dental offices that cannot stock dozens of product shades for financial or space reasons. It is ideal for any office that values a quick, easy system that creates attractive, functionally sound restorations.
Omnichroma does not attempt to match the value of the tooth shade the way other composites do by using pigments and dyes. Instead, Tokuyama Dental America debuts its Smart Chromatic Technology with this product. The material uses uniformly sized spherical filler particles, as do the other composites in the Tokuyama Dental product line; however, Omnichroma fillers change the way that light is transmitted. Ambient light is altered along the red-to-yellow area of the color spectrum, allowing it to match the color of the patient’s surrounding dentition. It includes UDMA/TEGDMA monomers and 260-nm silica and zirconia fillers.
Omnichroma material characteristics include high polishability, excellent handling, and resistance to ambient light effects, highlights of other Tokuyama Dental America’s Estelite products. Wear and abrasion properties, including wear of the composite and opposing tooth structure, are also excellent.
The Omnichroma paste is opaque-white prior to curing, making the material more visible for the clinician during manipulation. The application of a light source during curing causes the material to blend with the color of the surrounding tooth. A chamfered margin is suggested to make marginal borders disappear. A single shade is all that is needed to match most posterior and anterior teeth. A blocking agent (Omnichroma Blocker [Tokuyama Dental America]) is available for extensive Class III and Class IV restorations. The function of the blocker is to reduce shade-matching interference caused by other objects in the background of the mouth, including the tongue, gingiva, and cheek.
The author has had the opportunity to use Omnichroma for 4 months on dozens of restorations and has been extremely impressed by this innovative and revolutionary product. This article will share the restorative results achieved using this newly introduced composite on a variety of patients, aged 17 to 89, and with shades ranging from B1 to C4.
CASE REPORTS
Case 1
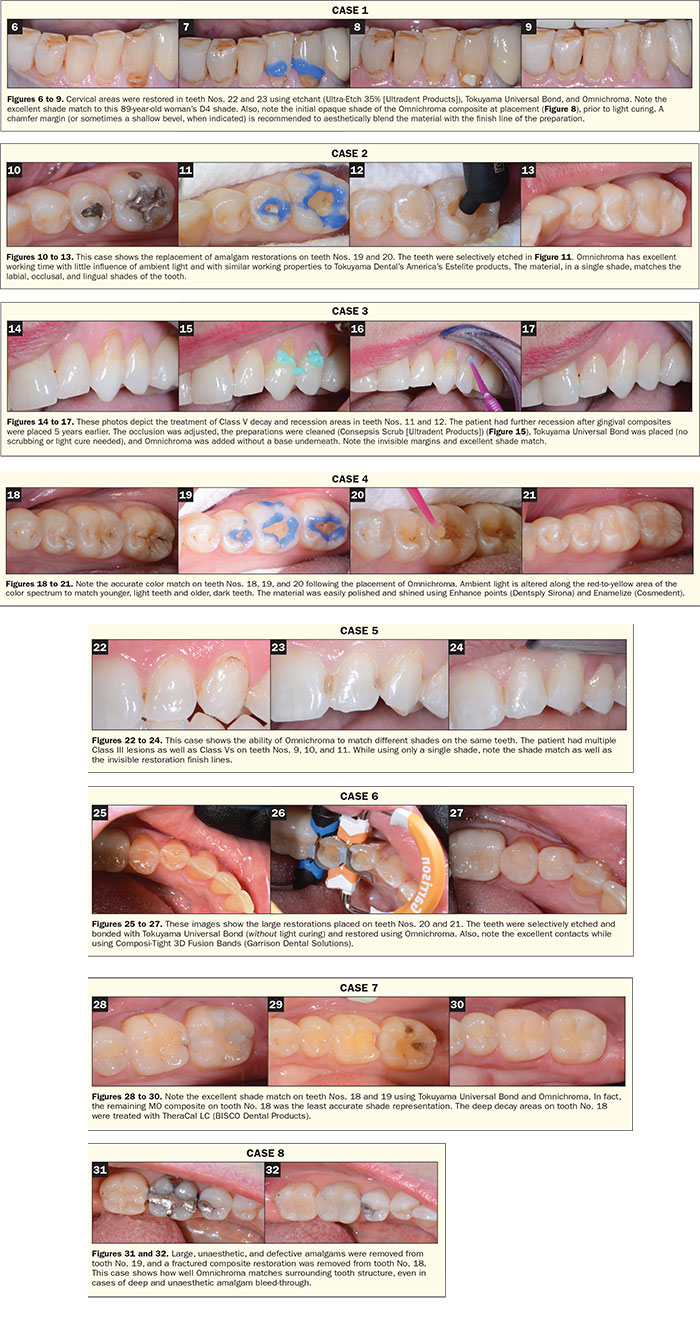
An 89-year-old female presented with Class V decay and erosion on teeth Nos. 22 and 23 (Figure 6).
The preoperative gingival shade was D4. Decay was removed. Then the preparation was cleansed (Consepsis Scrub [Ultradent Products]). The enamel was etched for 15 seconds (Ultra-Etch 35% [Ultradent Products]) (Figure 7), and Tokuyama Universal Bond parts A and B were mixed and applied to the enamel and dentin and air dried for 5 seconds. (Note: Tokuyama Universal Bond does not need to be light cured or scrubbed into the prepped tooth structure.) Omnichroma composite was applied and then light cured (Bluephase Style [Ivoclar Vivadent]) for 20 seconds. Note the white opaque shade of the dispensed material (Figure 8) and the final shade after curing (Figure 9). The restoration was finished and polished using Super-Snap Disks (Shofu Dental) and Jiffy Polishers (Ultradent Products). The excellent shade match can be seen in Figure 9.
Case 2
A 19-year-old female presented with amalgam restorations on teeth Nos. 19 and 20 and recurrent caries (Figure 10). The pre-op shade was A1. The amalgams were removed, and then the decay was excavated. The teeth were cleansed with Consepsis Scrub and selectively etched using Ultra-Etch 35% (Figure 11). Tokuyama Universal Bond was mixed and applied to the dentin and enamel as directed. Omnichroma was added using a PLT (compule) (Figure 12). The restoration was shaped using a 7406 gold-fluted bur (Microcopy) and polished using Enhance (Dentsply Sirona) polishing cups. Note the invisible margins and disappearance of amalgam bleedthrough (Figure 13).
Case 3
A 50-year-old female presented with cervical erosion and failing Class V fillings on teeth Nos. 11 and 12 (Figure 14). The pre-op shade was D2. Local anesthetic was administered, and the previously placed restorations and decay were removed. Consepsis Scrub was used to remove saliva and any other residue (Figure 15). The enamel was etched, and then Tokuyama Universal Bond was mixed and applied to the dentin and enamel as directed (Figure 16). Omnichroma was applied and cured for 20 seconds with the curing light. Polishing was accomplished using Super-Snap Disks and Groovy Diamond Polishing Brushes (CLINICIAN’S CHOICE Dental Products) and Enhance polishing cups. Note the accurate shade match (Figure 17).
Case 4
A 17-year-old male appeared with brown stains and decay on teeth Nos. 29, 30, and 31 (Figure 18). The pre-op shade was in the A1 range. The patient was anesthetized, decay was removed, and the enamel was etched using the selective-etch technique (Figure 19). The teeth were bonded using Tokuyama Universal Bond (Figure 20) and then air dried. The teeth were dried for 5 seconds, but not light cured, and Omnichroma was added and light cured. Note the excellent color match on all 3 teeth (Figure 21).
Case 5
A 30-year-old female wished to improve the appearance of her teeth prior to her wedding. She had not seen a dentist in 6 years and had many failing restorations and interproximal decay on many teeth (Figure 22). The pre-op shade was B1.
The patient was anesthetized, and decay was removed on teeth Nos. 9, 10, and 11 (Figure 23). The teeth were etched (Ultra-Etch 35%) and Tokuyama Universal Bond was placed as directed. Omnichroma Blocker was placed on the lingual cavity wall to prevent potential shade-matching interference from the lip, gingiva, or tongue. Omnichroma was then placed over all prepared areas, including over bevels that were placed to help eliminate unsightly finish lines. Note the material’s ability to blend with various shades on the same tooth (Figure 24).
Case 6
A 33-year-old female presented with multiple decay areas as well as erosion and abrasion areas on many teeth (Figure 25). The pre-op shade was B1. Omnichroma was used in this case to cover the sensitive dentin-exposed areas as well as interproximal decay. Teeth Nos. 20 and 21 were selectively etched and treated with Tokuyama Universal Bond. Matrix bands were placed (Composi-Tight 3D Fusion Bands [Garrison Dental Solutions]) (Figure 26). Omnichroma was placed as a DOL on tooth No. 21 and a DO restoration on tooth No. 20. The patient’s pre-op tooth shade matched extremely well with the single-shade Omnichroma (Figure 27).
Case 7
Note the pre-op shade issues for this patient (Figure 28). Composite restorations were planned for teeth Nos. 18 and 19. The small MO on tooth No. 18 was adequate and not removed. As seen in Figure 29, tooth No. 18 had very deep decay. TheraCal was placed at the deepest points. The tooth was selectively etched, and Tokuyama Universal Bond was placed and not light cured, pe
r manufacturer directions. The restorations were placed using Omnichroma and polished using Enhance and Enamelize (Cosmedent) kits. Note the excellent shade match on both teeth (Figure 30).
Case 8
Tooth No. 30, with a deep amalgam bleed-through, showed a positive shade match (Figures 31 and 32).
 |
CLOSING COMMENTS
The clear trend in dentistry over the past 30 years has been to create “tooth-specific” products that match an individual portion of a single tooth. Those products have become incrementally more accurate, especially as more and better shades have been developed. The one thing they have not been is simple to use. Prior to the introduction of Omnichroma, the thought of using a single composite that would match the shades of virtually every tooth was not a possibility. In the author’s opinion, this new direct composite material represents a revolutionary material advancement and will be an excellent option for nearly every dental office, hospital clinic, residency program, mission effort, and dental school.
References
- Buonocore MG. A simple method of increasing the adhesion of acrylic filling materials to enamel surfaces. J Dent Res. 1955;34:849-853.
- Schulein TM. Significant events in the history of operative dentistry. J Hist Dent. 2005;53:63-72.
- Sensi LG, Strassler HE, Webley W. Direct composite resins. Inside Dentistry. 2007;3:76.
- Radz GM. Direct composite resins. Inside Dentistry. 2011;7:108-114.
- Hervás-García A, Martínez-Lozano MA, Cabanes-Vila J, et al. Composite resins. A review of the materials and clinical indications. Med Oral Patol Oral Cir Bucal. 2006;11:E215-E220.
- Milnar FJ. The evolution of direct composites. Compend Contin Educ Dent. 2011;32:80-81.
- Simos S. Direct composite resin restorations: placement strategies. Dent Today. 2011;30:108-111.
- Lowe RA. Focus on: bioactive dental materials. Dent Today. 2017;36:16.
Dr. Auster completed 8 years in leadership positions at the American Academy of Cosmetic Dentistry (AACD). He is founder, past-president, and current director of the Greater New York Academy of Cosmetic Dentistry. Dr. Auster was named an AACD Humanitarian of the Year and recently completed his 10th year doing volunteer dentistry in Jamaica. He is a fellow of the American College of Dentists and was named a Dentistry Today Leader in Continuing Education for 2017 to 2019. He is a “Dawson Academy Scholar” and a Catapult Education KOL. Dr. Auster lectures internationally. He can be reached at (845) 364-0400 or via email at [email protected].
Disclosure: Dr. Auster received honoraria from Tokuyama Dental America for this article. He has previously received honoraria for seminars from Garrison Dental Solutions, Ivoclar Vivadent, COLTENE, Pulpdent, and Ultradent Products, Inc.
Related Articles
Universal Composite Matches All Patients’ Tooth Shades
Restorative Materials Continue to Evolve: Spherical Supra-Nano Composites
Composite Provides More Natural-Looking Bulk-Fill Restorations


