


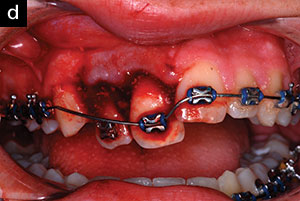
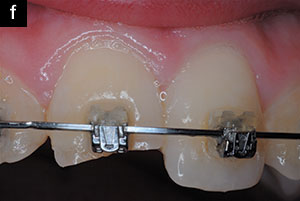
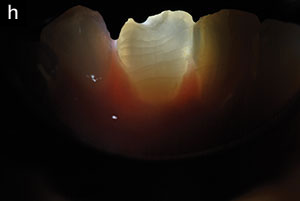
In the last 7 decades, there has been much interest in preventing dental injuries that occur during participation in sports.1-16 Teeth can be fractured and/or displaced by direct blunt force trauma or by a blow to the mandible that crunches the mandibular teeth traumatically against the maxillary teeth. Typical sports-related dental injuries in children and teens are shown in Figure 1.
The best type of tooth protection is a vacuum-formed mouthguard, custom made on a stone model of the maxillary arch. Pressure-laminated mouthguards provide an excellent fit and give particularly good protection.16-19 Using a slightly modified method, vacuum-formed mouthguards can even be made for patients in fixed orthodontic appliances.20 Some dentists, or their office auxiliaries, fabricate vacuum-formed mouthguards in their in-office labs. Others rely on commercial laboratories to make sports mouthguards using stone models, done by order of the clinicians via prescriptions.
When instructions are followed meticulously, the boil-and-bite (store-bought) mouthguards can also protect young athletes from sports-related dental injuries.5 These are often used when the expense of a vacuum-formed mouthguard made by the dentist or dental laboratory is prohibitive to the parent/guardian, or when a mouthguard is needed that can be rapidly generated in the family kitchen. However, the ability of parents and young athletes to fabricate boil-and-bite mouthguards varies greatly.
In some instances, a vacuum-formed mouthguard, or even a boil-and-bite mouth-formed device, may not be available. This can be due to expense or practicality. A custom mouthguard may be the most ideal, but for a child who is rapidly growing, and/or experiencing ever-changing tooth positions due to ongoing orthodontic treatment, a custom-formed device will usually not fit for an extended time period. Children and teens also frequently chew up their mouthguards during use, or lose them on the field or elsewhere. Continual replacements of these custom guards can be expensive and inconvenient for the parents.
 |
 |
 |
 |
 |
 |
 |
 |
 |
| Figure 1. Dental injuries in children and teens during sports activities. |
What can be used if a coach of a children’s field hockey, soccer, baseball, or basketball team has a number of players show up with no mouthguards, and the wise decision to use tooth protectors is also a mandatory one? What tooth protector is available when a child goes skateboarding, plays in a neighborhood basketball court, or in a touch football game, or has just been fitted with full-bonded orthodontic hardware which will be moving teeth such that custom-fitted mouthguards will not fit soon after?21,22 And what kind of mouthguard can a dentist give to a patient who just had injured teeth splinted into place, but insists on returning to the playing field?
In cases such as these, a tooth protector is needed that meets the following conditions:
- Is instantly available from the package to the mouth
- Can fit almost all children and teens because it adapts to small (6-year-old) and larger mouths (teenagers), including those with fixed orthodontic appliances, including palatal expanders
- Is comfortable and does not elicit gagging, and accommodates air exchange
- Can be sufficiently stable when the athlete occludes on the bite plane
- Is made of a soft, resilient material, approved for intraoral use, that can absorb impact and deflect traumatic forces directed at the teeth
- Protects both maxillary and mandibular teeth
- Can be attached to a helmet, if desired, by placing a lace through a breathing vent
- Can prevent crunching of the mandibular teeth against maxillary teeth in the case of a chin blow
- Is sanitary and inexpensive so periodic replacement is affordable and practical
- Even though comfortable to soft tissues, it has a bulk that is so large, that there is extremely low risk of swallowing or aspiration of the device.
 |
 |
| Figure 2. ToothShield (PRACTICON) tooth protector and impact deflector. | Figure 3. ToothShield in place in the mouth of a 13-year-old who was being treated with bonded orthodontic appliances. |
TOOTHSHIELD
ToothShield is marketed by PRACTICON as a patented tooth protector and impact deflector (Figure 2). It is manufactured (in the United States) from a thermoplastic elastomer; the same type that is used for pacifiers and nipples for baby bottles. The design includes posterior compression pads that compress the device inward, against the buccal surfaces of the posterior teeth, or attached orthodontic hardware (Figures 2 to 4). Inward compression accommodates smaller mouths, facilitated by v-shaped notches in the horizontal bite plane (Figure 2). Likewise, the notches allow for expansion, so the ToothShield spreads outward to fit larger arches. The internal aspects of the lips help stabilize the tooth protector in the anterior region, and a tilting maxillary anterior flange adapts to the labial vestibule by maxillary lip compression (Figures 3 and 5). The flange can be reduced in height with scissors, if it impinges the depth of the anterior vestibule in smaller mouths (Figure 6). In addition, a tether can be inserted for helmet attachment, if needed (Figure 7).
Informal questioning of children and teens using ToothShield have elicited only one complaint: as with any non-custom mouthguard, it can be awkward to speak with the device in place. However, the tongue and mandibular lip can stablize the ToothShield with the mouth slightly opened in order to accommodate shouting to a teammate or conversing on the field of play, as needed.
 |
 |
| Figure 4. Posterior compression pads stabilize the device. | Figure 5. ToothShield in cross section. Horizontal bite plane protects against chin blow, and tilting flange protects and stabilizes the unit. |
 |
 |
| Figure 6. To accommodate smaller mouths, one level can be cut from maxillary flange. | Figure 7. A lace tether can be inserted to attach to a helmet. |
CLOSING COMMENTS
Custom-fitted mouthguards are undoubtedly the optimal way to protect teeth from traumatic impact during sports activities. However, such mouthguards are not always available or affordable. ToothShields are adaptable to most children and teens, even to those wearing fixed orthodontic appliances, and can work as an acceptable alternative, when needed.
References
- Cathcart JF. Mouth protectors for contact sports. Dent Dig. 1951;57:346-348.
- Watts G, Woolard A, Singer CE. Functional mouth protectors for contact sports. J Am Dent Assoc. 1954;49:7-11.
- Merchant HW, Warren RW. Mouth protection in contact sports. Med Bull US Army Eur. 1955;12:53-55.
- Castaldi CR. Mouth guards in contact sports. J Conn State Dent Assoc. 1974;48:233-241.
- Castaldi CR. Sports medicine: The protective mouth guard. In: Castaldi CR, Brass GA. Dentistry for the Adolescent. Philadelphia, PA: WB Saunders; 1980:545-554, chapter 23.
- Castaldi CR. Sports-related oral and facial injuries in the young athlete: a new challenge for the pediatric dentist. Pediatr Dent. 1986;8:311-316.
- Castaldi CR. Sports dentistry. ASDC J Dent Child. 1989;56:236.
- Padilla R, Balikov S. Sports dentistry: coming of age in the ’90s. J Calif Dent Assoc. 1993;21:27-37.
- Padilla R, Dorney B, Balikov S. Prevention of oral injuries. J Calif Dent Assoc. 1996;24:30-36.
- Ranalli DN. Prevention of sports-related traumatic dental injuries. Dent Clin North Am. 2000;44:35-51, v-vi.
- Walker J, Jakobsen J, Brown S. Attitudes concerning mouthguard use in 7- to 8-year-old children. ASDC J Dent Child. 2002;69:207-211,126.
- ADA Council on Access, Prevention and Interprofessional Relations; ADA Council on Scientific Affairs. Using mouthguards to reduce the incidence and severity of sports-related oral injuries. J Am Dent Assoc. 2006;137:1712-1720.
- Chi HH. Properly fitted custom-made mouthguards. Compend Contin Educ Dent. 2007;28:36-40.
- Knapik JJ, Marshall SW, Lee RB, et al. Mouthguards in sport activities: history, physical properties and injury prevention effectiveness. Sports Med. 2007;37:117-144.
- American Academy on Pediatric Dentistry Clinical Affairs Committee; American Academy on Pediatric Dentistry Council on Clinical Affairs. Policy on prevention of sports-related orofacial injuries. Pediatr Dent. 2008-2009;30(suppl 7):58-60.
- Padilla RR, Lee TK. Pressure-laminated athletic mouth guards: a step-by-step process. J Calif Dent Assoc. 1999;27:200-209.
- Ranalli DN, Demas PN. Orofacial injuries from sport: preventive measures for sports medicine. Sports Med. 2002;32:409-418.
- Padilla RR. A technique for fabricating modern athletic mouthguards. J Calif Dent Assoc. 2005;33:399-408.
- Padilla R, Christensen GJ. Customized mouthguards for any sport [DVD]. pccdental.com/products/product/customized-mouthguards-for-any-sport.php. Accessed October 24, 2016.
- Croll TP, Castaldi CR. Custom sports mouthguard modified for orthodontic patients and children in the transitional dentition. Pediatr Dent. 2004;26:417-420.
- Salam S, Caldwell S. Mouthguards and orthodontic patients. J Orthod. 2008;35:270-275.
- Keim RG. Mouthguards and orthodontics. J Clin Orthod. 2010;44:9-10.
Dr. Croll maintains a private practice in Doylestown, Pa, specializing in pediatric dentistry. He is an affiliate professor in the department of pediatric dentistry at the University of Washington School of Dentistry in Seattle and an adjunct professor in the department of pediatric dentistry at the University of Texas Health Science Center at San Antonio. He can be reached at willipus@comcast.net.
Disclosure: Dr. Croll acknowledges financial interest in ToothShield by virtue of a patent licensing and royalty agreement with PRACTICON.
Related Articles
Mouthguard May Improve Athletic Performance in Addition to Protecting Teeth
Smart Mouthguard Detects Bruxism, Concussions, and More
Adherence to Guidelines After Dental Trauma Ensures More Positive Outcomes








