


INTRODUCTION
It is no secret that caring for children’s restorative needs in the dental office comes with challenges and unpredictability. Delivering successful restorative treatments for children is largely dependent upon 2 factors: what needs to be done for the health of a child, and what can be done, given the ability of the child to cooperate with the proposed procedure. Composite resin restorations are the most common restorations placed in North America. When placed properly and with isolation, they are a long-lasting aesthetic treatment option for children.1,2 The use of composite resin materials continues to skyrocket. As a result, the dental industry is filled with many material choices, all with their own individual benefits. Available to us are bulk-fill materials, bioactives, nano-hybrids, thermodynamics, different viscosities, distinctive enhanced mechanical properties, unique delivery systems, etc. The list of various attributes of different composite materials goes on and on.
Choosing the right composite resin restorative material must be based upon our patients’ needs and the properties of the materials. Obviously, when our patients are children, it is desirable to use materials and techniques that are efficient and effective. Ultimately, the success of a restoration in a child’s mouth depends upon proper diagnosis and the ability to deliver treatment with a selection of appropriate materials and techniques. Simplicity and success go hand in hand.
NEW RESTORATIVE MATERIALS
New materials have been introduced by Tokuyama Dental America. Omnichroma Flow and Omnichroma Blocker Flow (Tokuyama Dental America) have been launched as an expansion of resin-based Omnichroma restorative materials. Omnichroma is the world’s first one-shade universal composite capable of matching every patient, from A1 to D4, utilizing Tokuyama Dental’s “Smart Chromatic Technology.” As a result, workflow is streamlined as there is no need to shade match. Also, inventory and waste are reduced, as one shade of Omnichroma matches all patients. Omnichroma Blocker Flow serves to improve shade adaptation by preventing Omnichroma from picking up the oral cavity’s darkness and by masking stains or other discolored imperfections.
The introduction of flowable materials Omnichroma Flow and Omnichroma Blocker Flow now allows for the ability to restore with the advantages of this technology and the advantages of a flowable delivery system. Traditional packable composite resins have challenges and can be difficult to handle, requiring effort to adapt to cavity preparation walls. Traditional packable composites, when used alone, risk leaving voids in restoration fillings.3,4 Flowable composite resins, with their lower viscosities, adapt better to cavity preparations and have decreased incidence of voids when properly placed. Flowable composites are easier to handle and easier to deliver in hard-to-reach areas. In the past, flowable materials have traditionally had inconsistent compositions and, thus, variable mechanical and physical properties.5 First-generation flowable composite resin materials had mechanical properties that were very poor.6 This has left dental professionals with the misconception that all flowable composite materials are weak and inferior. However, now that paradigm must change. Tokuyama Dental has developed Omnichroma Flow and Omnichroma Blocker Flow to have all of the strength, versatility, and aesthetics that have been missing in the older flowable composites. These 2 products have enhanced aesthetic properties, high polishability, and stain resistance. Their physical-mechanical properties are also enhanced, with high flexural and compressive strength, low wear and abrasion, and low polymerization shrinkage. These materials can be placed easily and with confidence in the quality of the restoration. Omnichroma Flow and Omnichroma Blocker Flow have come to market, streamlining the delivery of dental restorations. Finally, there is a fast and simple way to restore.
 |
 |
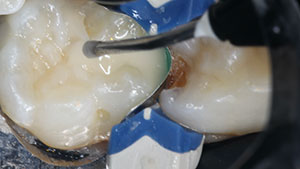
| Figure 1. Mesial carious lesion on tooth No. 75/K. | Figure 2. Preparation and removal of any soft, carious dentin. |
 |
 |
| Figure 3. Matrix placement using the Composi-Tight 3D Fusion Sectional Matrix System (Garrison Dental Solutions). | Figure 4. Selective-etch technique. |
Evidence is now guiding us to the use of flowable composite resin alone as a material for direct restoration of both Class I and Class II fillings. The direct restoration technique with flowable composite for primary molars has been described as a simple method to provide effective tooth-colored fillings, layering the flowable composite in increments. This fill technique, when used in primary molars, showed acceptable results in small to moderate cavities.7,8 In another clinical trial, heavily filled flowable composite resin materials have been shown to have equal success to packable composite materials.9 This substantiation and affirmation, as well as the evolution of improved materials, are guiding us to take advantage of this novel flowable resin material to simplify the placement of restorations in primary molars.
Guidelines for placement of direct restorations in primary dentition using flowable alone in an incremental fill should be followed to ensure success. First and foremost, there should be a proper treatment plan for your child patient and reliable and adequate anesthesia. After this, the single most important factor in success is isolation, either with a rubber dam or an isolation system: eg, DryShield or Isolite. Always be aware of the properties of the materials you are using and the inherent hydrophobicity of composite resins. Moisture contamination of a composite resin will lead to premature failure of your restoration. Next is proper clinical selection; composite resin restorations are successful in conservative-sized lesions. Care must be taken to remove all decay, leaving clean margins while not undermining the cusps or the buccal and lingual walls. If the lesion you are restoring is interproximal, care must also be taken to use a reliable sectional matrix system and, finally, to follow the manufacturer’s instructions for the restorative material you are using. Strict adherence to these principles will help to guarantee a quality result.
CASE STUDY
A 4-year-old patient with multiple caries was treatment planned for a full-coverage restoration and, in this case, would be restored with a prefabricated pediatric zirconia crown. Specifically for this case study, the focus will be upon the mesial carious lesion on teeth Nos. 75/K (Figure 1) and 74/L. The materials of choice for this case, Omnichroma Flow and Blocker Flow and a prefabricated pediatric zirconia crown (NuSmile), would fulfill both the function required and the aesthetics desired for this child and his or her parent.
The quadrant was isolated with a #27 Ivory rubber dam clamp and a black latex rubber dental dam (Sanctuary) in a slot-style isolation. Preparation was done with a #1116.8C FG single patient use NeoDiamond (Microcopy). Cavity design and preparation should be as conservative as possible while also allowing for sufficient depth of preparation to have enough bulk of material at a suitable thickness for the strength to resist the possibility of fracture. Simultaneously, care must be taken to ensure an adequate bulk of material to leave enough remaining tooth structure to maintain the integrity of the tooth. Attention must also be taken not to undermine any cusps while removing any infected dentin. The removal of any soft, carious dentin was accomplished with a large #8 slow-speed round bur (Figure 2).
The matrix of choice for this case is the Composi-Tight 3D Fusion Sectional Matrix System (Garrison Dental Solutions), and the rationale for the use of a sectional matrix system is as follows. Although, undoubtedly, interproximal contacts are improved when sectional matrices are used, the main rationale for using a matrix system with a ring is to maintain and properly isolate the gingival margin of the preparation and restoration. The placement of sectional matrices is of utmost importance for gingival margin integrity, prevention of leakage, and contamination of gingival crevicular fluids. In summary, the rationale for sectional matrix use in primary dentition is more for the adaptation of the matrix to the margins, allowing for less microleakage and greater longevity of the restoration (Figure 3).
A selective-etch technique with 35% phosphoric acid was used in this case and is the method of choice whenever possible. Using a selective-etch technique of applying phosphoric acid etch to enamel only using universal-type bonding agents enhances bond strength10,11 (Figure 4). Self-etch adhesive systems are very popular due to their ease of application and versatility. Tokuyama Universal Bond (Tokuyama Dental America) is a self-etch adhesive ideal for use in pediatric patients. It is a 2-bottle self-cure system. One drop from each of the bottles Bond A and Bond B is mixed in a well and applied over all surfaces to be bonded. Care must be taken to ensure that bond is placed on all surfaces of both enamel and dentin, including those hard-to-reach areas—for example, the gingival box. In cases of primary dentition, an appropriately sized microbrush must be chosen in order to reach these areas. Once all surfaces are coated, a weak stream of air (5 seconds), followed by a medium stream of air (5 seconds) is directed to the tooth to evaporate the solvent. No light curing is required as Tokuyama Universal Bond is a self-cure adhesive (Figure 5). Direct restoration follows. In this case, Omnichroma Blocker Flow was placed. Omnichroma Blocker Flow can be placed in increments of up to 2 mm and light cured (Figure 6).
 |
 |
| Figure 5. Self-etch adhesive system Tokuyama Universal Bond (Tokuyama Dental America). | Figure 6. Omnichroma Blocker Flow (Tokuyama Dental America) can be placed in increments of up to 2 mm and light cured. |
 |
 |
| Figure 7. Omnichroma Flow (Tokuyama Dental America) was also placed in increments of up to 2 mm and light cured. | Figure 8. An additional increment of Omnichroma Flow to replicate the marginal ridge. |
 |
| Figure 9. Omnichroma Blocker Flow and Omnichroma Flow blend seamlessly and are completely imperceptible. |
Following the placement of the blocker, the flow is placed, again in increments of up to 2 mm, and light cured (Figure 7). Since it is not possible to sculpt the flowable, I added an additional increment to replicate the marginal ridge (Figure 8). In primary dentition, detailed occlusal anatomy is not necessary for the form or function of the restoration. The final restoration, immediately postoperatively, is shown in Figure 9. Omnichroma Blocker Flow and Omnichroma Flow blend seamlessly and are completely imperceptible (Figure 9). (Note, as is evident in Figure 9, the interproximal contact will be modified once tooth No. 74/L is restored with the planned zirconia crown. This will be completed at the same appointment, but after placement of the composite restoration so as not to contaminate composite restoration placement with any excess hemorrhage created during preparation of the prefabricated pediatric zirconia crown.)
CONCLUSION
Caring for children in a dental office doesn’t need to be stressful. Choosing appropriate techniques and dental materials is necessary for both simplicity and success. Patient- and parent-centered care and the marriage of methods and materials will always lead to favorable outcomes.
References
- Bücher K, Tautz A, Hickel R, et al. Longevity of composite restorations in patients with early childhood caries (ECC). Clin Oral Investig. 2014;18(3):775–82. doi:10.1007/s00784-013-1043-y
- Pinto Gdos S, Oliveira LJ, Romano AR, et al. Longevity of posterior restorations in primary teeth: results from a paediatric dental clinic. J Dent. 2014;42(10):1248–54. doi:10.1016/j.jdent.2014.08.005
- Opdam NJ, Roeters JJ, Peters TC, et al. Cavity wall adaptation and voids in adhesive Class I resin composite restorations. Dent Mater. 1996;12(4):230–5. doi:10.1016/s0109-5641(96)80028-5
- Opdam NJ, Roeters JJ, Joosten M, et al. Porosities and voids in Class I restorations placed by six operators using a packable or syringable composite. Dent Mater. 2002;18(1):58-63. doi:10.1016/s0109-5641(01)00020-3
- Baroudi K, Rodrigues JC. Flowable resin composites: a systematic review and clinical considerations. J Clin Diagn Res. 2015;9(6):ZE18-24. doi:10.7860/JCDR/2015/12294.6129
- Bayne SC, Thompson JY, Swift EJ Jr, et al. A characterization of first-generation flowable composites. J Am Dent Assoc. 1998;129(5):567–77. doi:10.14219/jada.archive.1998.0274.
- Bücher K, Metz I, Pitchika V, et al. Flowable composite as a direct restoration technique for primary molars. Eur J Paediatr Dent. 2017;18(3):243-246. doi:10.23804/ejpd.2017.18.03.13
- Attar N, Turgut MD, Güngör HC. The effect of flowable resin composites as gingival increments on the microleakage of posterior resin composites. Oper Dent. 2004;29(2):162–7. https://pubmed.ncbi.nlm.nih.gov/15088727/
- Rocha Gomes Torres C, Rêgo HM, Perote LC, et al. A split-mouth randomized clinical trial of conventional and heavy flowable composites in class II restorations. J Dent. 2014;42(7):793–9. doi:10.1016/j.jdent.2014.04.009
- Rosa WL, Piva E, Silva AF. Bond strength of universal adhesives: A systematic review and meta-analysis. J Dent. 2015;43(7):765–76. doi:10.1016/j.jdent.2015.04.003
- Lenzi TL, Guglielmi Cde A, Umakoshi CB, et al. One-step self-etch adhesive bonding to pre-etched primary and permanent enamel. J Dent Child (Chic). 2013;80(2):57-61.
Dr. Cohn is a general dentist, devoted solely to the practice of dentistry for children. She maintains a private practice at Kids Sleep Dentistry Winnipeg and Western Surgery Centre in Winnipeg, Man, Canada. She is proud to be a member of the American Academy of Pediatric Dentistry Speakers Bureau and the Pierre Fauchard Academy and a co-founder of the Women’s Dental Network. Dr. Cohn has been named as one of Dentistry Today’s Leaders in Continuing Education multiple years in a row. She has published several articles and conducted webinars. She enjoys lecturing on all aspects of children’s dentistry for the general practitioner, both nationally and internationally. She can be reached at drcohn@shaw.ca.
Disclosure: Dr. Cohn has received an educational grant from Tokuyama Dental America.
Related Articles
Silver Modified Atraumatic Restorative Technique for Pediatric Patients
Pediatric Dentistry Should Focus on Caries Prevention
Efficient Placement of Composite Restorations








