


Edentulous patients who are resigned to using conventional complete dentures may experience many negative issues affecting their overall health and psychological well-being. Methods to improve chewing ability can positively affect the digestive process, providing better nutrition to the patient. Dental implant overdentures have proven to be a viable alternative to conventional dentures and are now able to be a cost-effective treatment modality for many of our patients. Also important is the indication that implants that support an overdenture help preserve residual bone.1 Our patients need to be aware that over time, as their teeth are lost, the bone will resorb, which will require conventional dentures to be relined or necessitate the use of denture adhesives to retain their appliances. Correctly placed and integrated dental implants may minimize this bone loss.
Educating our patients as to the benefits of implant therapy is within the realm of the general dentist, and providing this mode of therapy is both financially and professionally rewarding.
A Viable Treatment Option
Implant-retained overdentures have proven to be a viable treatment option for patients who request improved denture stability and chewing function. The design of these overdentures has evolved over the years. At one time, cast bars with attachments were fabricated. This proved to be an expensive treatment modality and relied on the technical skills of the technician. Casting has been replaced with CAD/CAM milling protocols, which help establish a passive fit over the integrated dental implants. The most critical aspects of any implant-retained overdenture are proper positioning in the edentulous arch and the angulation of the dental implants themselves. Spacing anterior-posteriorly will help prevent rocking of the prosthesis during chewing function.2
 |
=Attachment systems can be divided into factors such as retention, durability, patient requests, and technical simplicity. There have been many retentive designs including magnets, O-rings, bars, Ceka, ERA, and Hader clips used over the years. Connecting bars were often used to attach implants, especially if they were significantly divergent. Each may have had advantages and disadvantages for the patient and the dentist.3
Cost and simplicity are 2 important factors in deciding to use the LOCATOR Implant Attachment System (Zest Dental Solutions) to provide denture stability to our patients.
LOCATOR attachments are long-lasting, with about 60,000 cycles of use. The patient is advised to have the implants and prostheses checked periodically, with the attachments changed out approximately once per year.4
Many dentists rely on laboratory technicians to create denture prostheses and underlying retentive designs. With the advent of LOCATOR attachments, used in conjunction with dental implants, we are able to provide outstanding form and stability for our patients at a reasonable cost. The investment by the patient in this treatment is found to be acceptable in many circumstances.
The quality of life created by eliminating full palatal coverage and creating a prosthesis that increases chewing efficiency and eliminates the need for any denture adhesive is remarkable.
These implant-retained overdentures are a very affordable and viable option to achieve improved function and maintain lip support and function. Not only do these prostheses require a limited number of dental implants to effectively retain removable appliances, they are also easy for the patient to maintain over time. The problems with conventional full-arch complete dentures are that they often result in triggering a gagging reflex and the taste buds on the roof of the mouth are covered. Retention is sometimes challenging, requiring different denture adhesives.
When dental implants are properly positioned in either the maxillary or mandibular arch, and have minimal divergence within the arch, the LOCATOR attachments provide a cost-effective and retentive means to maintain the implant-retained overdentures.
However, it is imperative that the LOCATOR attachments be processed properly, otherwise the retentive rings seem to wear out quickly, frustrating both the patient and the dentist. Most dentists would prefer dental laboratories to process LOCATOR attachments in overdentures out of simple convenience. The dental lab needs to process the attachments on a hard, final cast. This may not provide a complete seat on the soft tissue because these implant-retained overdentures are both implant- and tissue-supported.
Proper Positioning and Seating of Attachments
The best method to ensure proper positioning and seating of LOCATOR attachments is to cold cure them chairside. This procedure may initially seem complicated, but once the steps are understood, the results will be consistent.
The LOCATOR implant attachment system is designed for use with overdentures or partial dentures, retained in whole or in part by endosseous implants in the mandible or maxilla.
They provide the lowest vertical height available. The attachment is 2.5 mm on a non-externally hexed dental implant. They have a self-locating design, which allows the patient to easily seat the overdentures without the need for an accurate alignment of the attachment components. They either seat or do not. The dual-retention system provides the LOCATOR attachment with a significant retention surface area. The inside and outside retention allows for a long-lasting retentive device. The pivoting LOCATOR attachment allows for a resilient connection of the overdenture without any resulting loss of retention. The retentive nylon attachment remains completely in contact with the abutment socket, while its titanium denture cap has a complete range of rotational movement over the male LOCATOR extension. LOCATOR attachments are used to restore implants with up to a 10° divergence, or 20° between 2 implants. However, the extended-range replacement males can accommodate a divergence between 10° and 20°, or 40° between implants.
 |
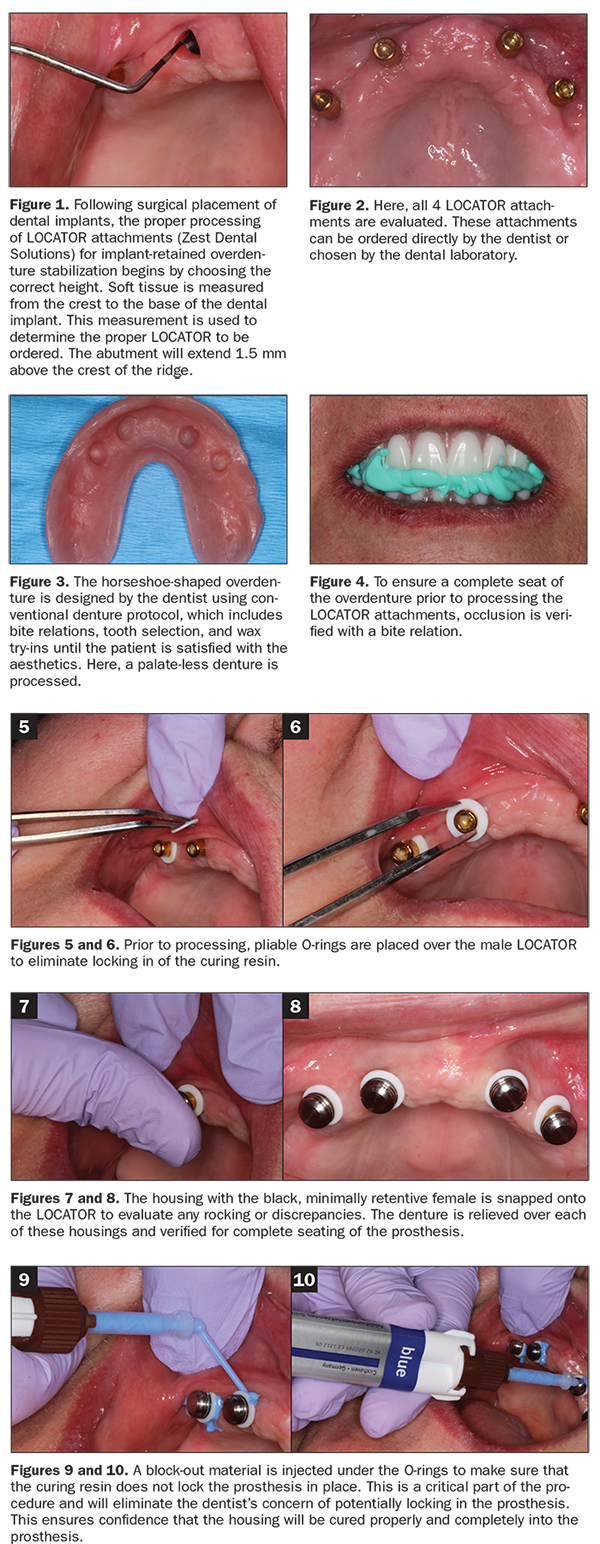
After the type of implant and diameter are determined, the proper LOCATOR attachment is chosen. The height of the attachment is measured from the coronal portion of the implant body to the contour of the soft tissue (Figure 1). The height of the LOCATOR attachment chosen is determined by the tissue height. The actual height of the LOCATOR male will be 1.5 mm taller than that measurement (Figure 2).
When uncovering the implants, one must make sure that tissue and excess bone are removed from around the coronal portion of the implant. This will ensure that the attachment seats passively. The abutment is then torqued to 35 Ncm.
The abutment driver engages the inside diameter of the LOCATOR and is used to thread it into the implant body. Torque the abutment to 30 Ncm to prevent its loosening upon constant use. Once the attachment is cured into the overdenture itself, the try-in nylon attachment is removed and replaced with a more retentive device. These include attachments of various retention: clear (5 lbs), pink (3 lbs), and/or blue (1.5 lbs). If the divergence of the implants is between 10° and 20°, the extended-range replacement males can be considered: green (4 lbs), orange (2 lbs), or red (1 lb). These can accommodate divergent implants up to 20° (or 40° between implants).
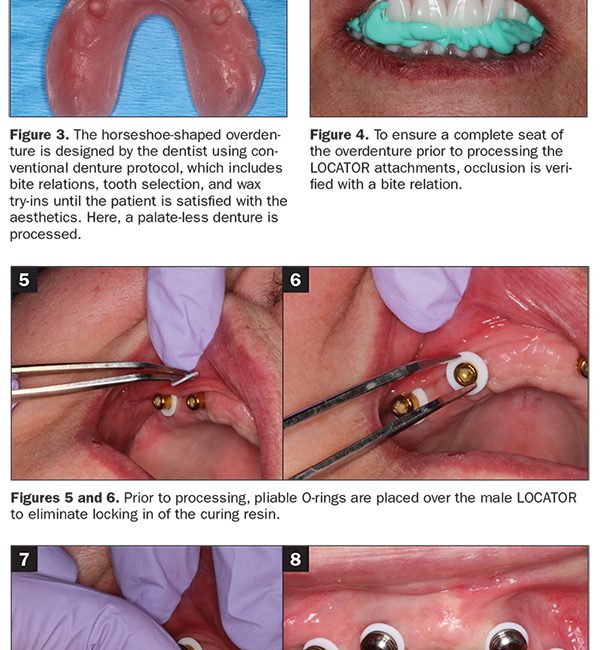
A horseshoe-shaped overdenture is designed using conventional denture protocol, which includes bite relations, tooth selection, and wax try-ins, until the patient is satisfied with the aesthetics. In Figure 3, a palate-less denture was processed. To ensure a complete seat of the overdenture prior to processing the LOCATOR attachments, occlusion is verified with a bite relation. Chairside processing of the female housing and retentive device is the most reliable method of proper stabilization (Figure 4). If the dental lab processes the housing, they have to accommodate not only the ridged LOCATOR male abutment but also the soft tissue.
Preventing Inaccuracies of the Final Prosthesis
Implant overdentures are both hard- and soft-tissue retained, so any movement of the soft tissue can result in inaccuracies of the final prosthesis. Note that dental laboratory-processed LOCATOR attachments often result in an incomplete seating of each of the 4 housings, which may result in movement or excessive wearing of one or more of the attachments.
To begin, place the attachments onto the LOCATOR abutments and make sure they snap on completely. Relieve the underside of the denture appropriately so there is no contact or rubbing. Check the passive fit by using bite relation material in each relieved area. Occlusal paper, occlusal spray, fit tester material, or even toothpaste can also be used to verify there is a totally passive fit over the LOCATOR abutments. It is imperative that the attachments do not touch the denture base. Relieve enough to create at least a 2-mm gap. Passive seating is done with the Fit Test. Complete seating of the denture over the abutments and attachments is critical and is first done by making an interocclusal bite relation with conventional bite registration polyvinylsiloxane material.
Next, place the disposable O-ring, which serves as a block out component around the abutments in the mouth (Figures 5 and 6). The metal housing, with the black, minimally retentive female in a metal housing, is snapped onto the LOCATOR to evaluate any rocking or discrepancies. The denture is relieved over each of these housings and verified for complete seating of the prosthesis (Figures 7 and 8).
Block out the cervical portion with the Fit Test PVS material (VOCO) to ensure that no undercuts are available to lock in the overdenture once the acrylic is cured (Figures 9 and 10). Flow and dry the adhesive into each relieved receptacle on the underside of the denture (Figure 11). Mix and syringe the self-cure Quick Up material (VOCO) about two-thirds into each of the prepared receptacles in the underside of the denture (Figure 12). Passively place the denture in the patient’s mouth, making sure that the occlusion is correct and the denture has a complete seat. This is verified by having the patient occlude into the bite registration made prior to seating the LOCATOR attachments. Remember the implant-retained overdentures are both implant and soft-tissue supported. Remove the denture and the attachments from the mouth after 2.5 minutes (Figure 13). Repair any voids or defects with the light-cured Quick UP LC flowable material (VOCO). Polish any flash with acrylic finishing and polishing burs (Figure 14).
Figure 15 illustrates when the black housings are removed and the final retentive attachments are replaced. These will snap to position. The LOCATOR core tool is used to remove the male from the metal denture cap, or a sharp scaler can be used. It is also used to snap the new attachment into the housings. The newly processed LOCATOR attachments are then polished (Figure 16). The denture will now snap into place, providing the patient with outstanding retention, stability, and function with this horseshoe-shaped, implant-retained overdenture (Figures 17 to 19). The denture seat is then verified, and form and function has been provided for the patient (Figure 20).
Sometimes food and debris can accumulate inside the LOCATOR attachment, so it is imperative that the patient be instructed on removing any material from inside the male attachment. This is accomplished with proper and thorough brushing, and a Waterpik (Water Pik) is also helpful. Toothpaste works well to reduce plaque on the inside of the attachments.
CONCLUSION
Implant-retained overdentures have proven to be a cost-effective and excellent treatment choice for many of our edentulous patients. Two to 4 implants are strategically placed to provide stability of a denture and create retention. They are fairly easy to maintain, and the dentures can be removed by the patient for easy cleaning. Function and chewing ability are significantly improved, and the patient’s quality of life is elevated. LOCATOR-attached overdentures make for a cost-effective and relatively simple retentive device. If retention needs to be improved, the nylon inserts are easy to change. Not all patients require, request, or are financially able to afford the most popular fixed, implant-retained bridges. However, the implant-retained prosthesis appears to be an ideal improvement over conventional dentures.
References
- Martínez-Lage-Azorín JF, Segura-Andrés G, Faus-López J, et al. Rehabilitation with implant-supported overdentures in total edentulous patients: a review. J Clin Exp Dent. 2013;5:e267-e272.
- Misch CE. Contemporary Implant Dentistry. 3rd ed. St. Louis, MO: Mosby Elsevier; 2008.
- Mahajan N, Thakkur RK. Overdenture Locator attachments for atrophic mandible. Contemp Clin Dent. 2013;4:509-511.
- The Locator: useful attachment for overdentures. Dental News. http://www.dentalnews.com/2015/07/03/the-locator-useful-attachment-for-overdentures/. Accessed March 27, 2020.
Dr. Kosinski received his DDS degree from the University of Detroit Mercy School of Dentistry (Detroit Mercy Dental) and his Mastership in Biochemistry from the Wayne State University School of Medicine. He is an affiliated adjunct clinical professor at Detroit Mercy Dental, currently serves as the associate editor of the AGD journals, and was recently named implants editor at Dentistry Today. He is a past president of the Michigan Academy of General Dentistry. Dr. Kosinski is a Diplomat of the American Board of Oral Implantology/Implant Dentistry, the International Congress of Oral Implantologists (ICOI), and the American Society of Osseointegration. He is a Fellow of the American Academy of Implant Dentistry and received his Mastership in the AGD. He can be reached at drkosin@aol.com.
Dr. Tilley is a graduate of the University of Alabama School of Dentistry. A native of Pensacola, Fla, she has been practicing dentistry in her hometown since 1998. Dr. Tilley keeps up with the latest in dentistry by attending continuing education seminars on topics such as oral surgery, implants, veneers, periodontal disease, cosmetic procedures, and much more. She has also done extensive training at the Las Vegas Institute and the Engel Institute with Drs. Timothy Kosinski and Todd Engel. She is a member of the AGD, the ADA, the Florida Dental Association, the Alabama Dental Association, the Academy of Laser Dentistry, the ICOI, and the Academy of American Facial Esthetics. She has published extensively on implant dentistry techniques, lasers, and Botox/fillers. She can be reached at stephflynntilley@cox.net.
Disclosure: The authors report no disclosures.
Related Articles
Rising Demand Drives Need for Dental Implant Education
Tooth Extractions and Bone Grafting
Proper Preparation for Prosthetically Driven Implants: CBCT Diagnosing and Surgical Protocol








