
MAINTENANCE PROBLEMS
 |
|
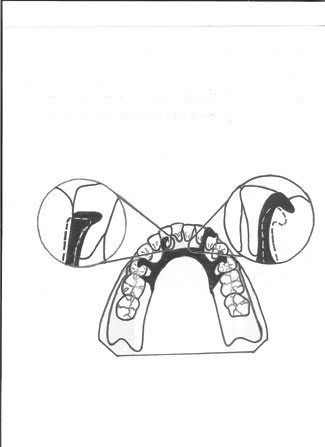
Figure 1. Cingulum or incisal rests drift away from the teeth, resulting in gaps. |
 |
|
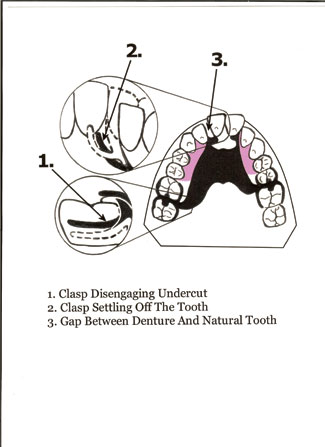
Figure 2. If a partial denture is not maintained, it may become unsalvageable. |
 |
 |
|
Figure 3. A partial denture case that experienced settling due to loss of ridge support. |
Figure 4. This neglected partial denture is beyond repair. |
As can be seen in Figure 2, if the partial is not maintained, after a certain point it becomes unsalvageable. After the ridge support lessens and the partial begins to settle, as illustrated by No. 1 in Figure 2, the clasps on the most distal abutments begin to disengage the undercuts, and spaces between the rests and the teeth develop. Illustrated by No. 2 in Figure 2, the clasp on the central incisor begins to settle downward and becomes non-retentive. If the doctor attempts to restore the retention by adjusting the clasp, the severity of the undercut will prevent the partial from seating, or after a painful snap, from being removed from the mouth. Illustrated by No. 3 in Figure 2, the cingulum rests will settle off both centrals, and a diastema and a drop between the right central incisor and the denture tooth will develop. Figure 3 shows a model of an actual case that has experienced such settling. Since the I bar clasp on the right central has settled off the tooth and was impinging on the tissue, the doctor removed it. As seen in Figure 4, this patient has neglected the partial for too long, and repairing it was no longer an option.
 |
 |
|
Figure 5. This lower partial denture (model) was neglected and needed relining for years. The patient could no longer wear it due to impingement on the tissue. |
Figure 6. Occlusal view of partial denture (model) shown in Figure 5. |
MAINTENANCE PLAN
After the finished partial is delivered to the patient and the final adjustment is made, a personalized maintenance plan for the patient needs to be prescribed. As part of a 6-month office visit, changes in the ridge should be monitored. This is best accomplished by examining the following:
Contacts Between the Denture and Opposing Teeth
Contacts between the denture teeth and the opposing teeth are best determined by placing articulating paper no thicker than 0.0008 of an inch, or 20 µm, between the opposing quadrants and pulling the paper with the teeth in centric. Every tooth should catch the paper. If it is determined that the contacts have loosened, it is a sign that the edentulous ridge is beginning to change.
Space Underneath the Saddle Base and Ridge
Retention of the Clasps
Mr. Saunaitis is a former dental laboratory owner, educator, publisher, and researcher. With more than 25 years of experience, he has developed techniques that better integrate crowns, bridges, and implants with the removable sector of dental technology. He has been published in various dental journals and newspapers and has appeared on radio and television. He has combined much of his research into a full-day slide presentation entitled “Forum for Prosthetic Dentistry.” To be notified about upcoming events or to reach the author, e-mail [email protected]

