


 |
| Figure 1. The Canary System. |
INTRODUCTION
Detecting cracks in teeth is one of the more challenging clinical situations. The “cracked tooth syndrome” was described more than 40 years ago,1 and clinicians still struggle to detect cracks early and to provide appropriate therapy. Patients usually present with vague symptoms, such as acute pain upon mastication of grainy and tough foods, and sharp brief pain with cold stimulus. These findings relate to cusp fracture, but there can also be other symptoms associated with a crack/fracture, such as slight to severe pain consistent with irreversible pulpitis, or pulpal necrosis. Periapical and bite-wing radiographs usually cannot image the crack or fracture. So the dilemma is how one detects, and then manages cracks/fractures in teeth.
This article will present a case report involving the use of the latest technology for the detection of a crack in a mandibular first molar.
Predisposing Factors to Cracked Teeth
A number of papers indicate that cracked teeth were associated with intracoronal restorations and frequently found in mandibular molars.2-5 The most commonly identified etiologic factor was the design of the cavity preparations. Large restorations, inappropriate use of pins, restorations encroaching upon the marginal ridges or undermining the marginal ridges are some of the factors. Selection of restorative materials may also be a factor. Bonded restorations may possibly reduce the incidence of cracks or fractures. Bruxism and other parafunctional habits, wear, malocclusion, steep cuspal inclines, or deep occlusal grooves were also considered as predisposing factors.6-9 Cracks may also occur in intact teeth with no restorations. One study found that 28% of the longitudinal fractures occurred in teeth with no restorations,10 while another study of 154 cases found that 60.4% had no restorations and a further 29% had only Class I restorations.11
New Technology Introduced
New diagnostic tools are coming to market that can help to image and detect defects in the crystal structure of the tooth which are associated with cracks and fractures. One of these technologies, The Canary System (Figure 1), uses the energy conversion technology, called photothermal radiometry-luminescence (PTR-LUM), to image and examine the tooth. Pulses of laser light are shone on the tooth and the laser light is converted to heat (PTR) and light (LUM), which are emitted from the tooth surface when the laser is off. These harmless pulses of laser light allow a clinician to examine subsurface caries up to 5 mm below the surface.12,13 Carious lesions modify the thermal properties (PTR) and glow (LUM) from the healthy teeth. As a lesion grows, there is a corresponding change in the signal as the heat is confined to the region with crystalline disintegration (dental caries) and PTR increases and LUM decreases. As remineralization progresses and enamel prisms begin to reform their structure, the thermal and luminescence properties begin to revert back in the direction of healthy teeth.14-16 The system is so sensitive it detects very small changes in temperature (less than 1°C to 2°C); much less than that generated by a conventional dental curing light. These changes in temperature are imperceptible to the patient.
The Canary Number (ranging from zero to 100) is created from an algorithm combining the PTR and LUM readings and is directly linked to the status of the enamel or root surface crystal structure.17 A Canary Number of less than 20 indicates a healthy tooth surface. A Canary Number greater than 70 indicates a large lesion that may justify restoration. Canary Numbers falling between 20 and 70 indicate the presence of an early carious lesion or crack that doesn’t require a restoration but can be remineralized.18 The treatment decisions are based upon the type of remineralization treatment, position of the lesion, and overall risk of developing caries including oral hygiene.
Research has demonstrated that PTR-LUM technology used in The Canary System can detect:
- Occlusal pit-and-fissure caries19,20
- Smooth-surface caries21,22
- Acid erosion lesions12,23
- Root caries24,25
- Interproximal carious lesions13,26
- Beneath fissure sealants27
- Beneath the intact margins of composite resins28
- Demineralization and remineralization of early carious lesions24,29-31
Photothermal radiometry-luminescence technology allows clinicians to detect small early lesions in order of 50 µm in depth up to 5 mm below the tooth surface, even in the interproximal regions of teeth.32 It provides a repeatable measurement that is linked to the status of the enamel or root surface under examination.
CASE REPORT
A 53-year-old male presented complaining of tooth-borne pain upon cold stimulus during the previous 4 days. Upon examination, we could not localize the pain, and there was no pain on percussion. A bite-wing radiograph (Figure 2), taken at a recare visit 6 weeks previously, showed shallow occlusal amalgam restorations on the mandibular first and second molars. A periapical radiograph (Figure 3), taken at the time of the appointment, showed a large extensive amalgam restoration on the mandibular third molar, with a possible radiolucency associated with the mesial root. There was pain upon cold stimulus on all the mandibular right molars; however, it was most severe on the third molar. A recommendation was made to have this tooth extracted or endodontically treated.
 |
 |
| Figure 2. Bite-wing radiograph (right side), taken at a recare appointment 6 weeks prior to the first occurrence of pain, showing the mandibular molars. | Figure 3. Periapical radiograph (right side) taken at the first emergency visit. |
 |
| Figure 4. Photograph of the mandibular right posterior quadrant. |
 |
| Figure 5. Canary Scan results. |
 |
| Figure 6. Removal of the amalgam, showing caries and a crack; with the corresponding Canary Numbers. |
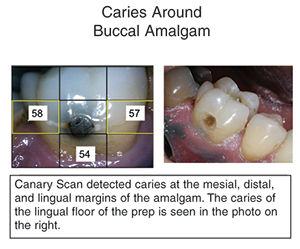 |
| Figure 7. Canary Scan of the buccal amalgam. |
The patient returned 3 days later and reported that the pain was now more localized to the mandibular first molar. Upon examination, the pain was more pronounced over the first molar. Photographs (Figure 4) were taken of the tooth and a Canary Scan done of both the occlusal and buccal surfaces.
The Canary Scan (Figure 5) showed Canary numbers of 58 associated with the mesial marginal ridge; 36 with the distal marginal ridge; and 97 with the lingual border of the occlusal amalgam. Upon removal of the amalgam (Figure 6), cracks were seen in both mesial and distal marginal ridges. There was also a substantial amount of recurrent caries around the lingual margin of the restoration.
The caries was removed from the lingual aspect. The cracks and caries along the mesial and distal marginal ridges were removed. A bonded mesial occlusal distal composite was placed.
A Canary Scan was done on the buccal amalgam on this tooth (Figure 7), indicating the presence of caries around the restoration. Upon removal of the amalgam, caries was indeed found and a new composite restoration was placed.
IN SUMMARY
Detection of cracks in teeth is a very challenging task. At times, the symptoms may not be indicative of the presence of a crack. In addition, bite-wing and periapical radiographs may not be able to image small microfractures. As a result, the clinician can be greatly assisted with technology that can directly examine the crystal structure of the tooth to detect any voids or porosities. The Canary System, using its PTR-LUM technology, provides the clinician with a diagnostic device to detect caries and cracks around the margins of restorations.
References
- Cameron CE. Cracked-tooth syndrome. J Am Dent Assoc. 1964;68:405-411.
- Cameron CE. The cracked tooth syndrome: additional findings. J Am Dent Assoc. 1976;93:971-975.
- Bader JD, Martin JA, Shugars DA. Preliminary estimates of the incidence and consequences of tooth fracture. J Am Dent Assoc. 1995;126:1650-1654.
- Rosen H. Cracked tooth syndrome. J Prosthet Dent. 1982;47:36-43.
- Bader JD, Martin JA, Shugars DA. Incidence rates for complete cusp fracture. Community Dent Oral Epidemiol. 2001;29:346-353.
- Braly BV, Maxwell EH. Potential for tooth fracture in restorative dentistry. J Prosthet Dent. 1981;45:411-414.
- Gher ME Jr, Dunlap RM, Anderson MH, et al. Clinical survey of fractured teeth. J Am Dent Assoc. 1987;114:174-177.
- Homewood CI. Cracked tooth syndrome—incidence, clinical findings and treatment. Aust Dent J. 1998;43:217-222.
- Ratcliff S, Becker IM, Quinn L. Type and incidence of cracks in posterior teeth. J Prosthet Dent. 2001;86:168-172.
- Seo DG, Yi YA, Shin SJ, et al. Analysis of factors associated with cracked teeth. J Endod. 2012;38:288-292.
- Roh BD, Lee YE. Analysis of 154 cases of teeth with cracks. Dent Traumatol. 2006;22:118-123.
- Jeon RJ, Phan TDT, Wu A, et al. Photothermal radiometric quantitative detection of the different degrees of demineralization of dental enamel by acid etching. J Phys IV France. 2005;125:721-723.
- Jeon RJ, Matvienko A, Mandelis A, et al. Detection of interproximal demineralized lesions on human teeth in vitro using frequency-domain infrared photothermal radiometry and modulated luminescence. J Biomed Opt. 2007;12:034028.
- Matvienko A, Jeon RJ, Mandelis A, et al. Photothermal detection of incipient dental caries: experiment and modeling. Proc SPIE. 2007;6759.
- Jeon RJ, Hellen A, Matvienko A, et al. Experimental investigation of demineralization and remineralization of human teeth using infrared photothermal radiometry and modulated luminescence. Proc SPIE. 2008;6856.
- Matvienko A, Mandelis A, Abrams S. Robust multiparameter method of evaluating the optical and thermal properties of a layered tissue structure using photothermal radiometry. Appl Opt. 2009;48:3192-3203.
- Garcia JA, Mandelis A, Abrams SH, et al. Photothermal radiometry and modulated luminescence: applications to dental caries detection. In: Popp J, Tuchin VV, Chiou A, et al, eds. Handbook of Biophotonics. Volume 2: Photonics for Health Care. Weinheim, Germany: Wiley-VCH; 2011:1047.
- Abrams S, Sivagurunathan K, Jeon RJ, et al. Multi-center clinical study to evaluate the safety and effectiveness of ‘The Canary System’ (PTR-LUM Technology) [ORCA Congress abstract 32]. Caries Res. 2011;45:187.
- Jeon RJ, Han C, Mandelis A, et al. Diagnosis of pit and fissure caries using frequency-domain infrared photothermal radiometry and modulated laser luminescence. Caries Res. 2004;38:497-513.
- Jeon RJ, Mandelis A, Sanchez V, et al. Dental depth profilometric diagnosis of pit and fissure caries using frequency-domain infrared photothermal radiometry and modulated laser luminescence. Proc SPIE. 2004;5320.
- Jeon RJ, Mandelis A, Sanchez V, et al. Nonintrusive, noncontacting frequency-domain photothermal radiometry and luminescence depth profilometry of carious and artificial subsurface lesions in human teeth. J Biomed Opt. 2004;9:804-819.
- Jeon RJ, Mandelis A, Abrams SH. Depth profilometric case studies in caries diagnostics of human teeth using modulated laser radiometry and luminescence. Rev Sci Instrum. 2003;74:380-383.
- Abrams SH, Matvienko A, Ye V, et al. Detection and monitoring of dental erosion using PTR-LUM. Presented at: IADR General Session; March 17, 2011; San Diego, CA. Abstract 238.
- Jeon RJ, Hellen A, Matvienko A, et al. Detection of demineralized-remineralized lesions on root and enamel of human teeth in vitro using infrared photothermal radiometry and modulated luminescence [ORCA Congress abstract 157]. Caries Res. 2007;41:323.
- Jeon RJ, Hellen A, Matvienko A, et al. In vitro detection and quantification of enamel and root caries using infrared photothermal radiometry and modulated luminescence. J Biomed Opt. 2008;13:034025.
- Jeon RJ, Matvienko A, Mandelis A, et al. Interproximal dental caries detection using Photothermal Radiometry (PTR) and Modulated Luminescence (LUM). Eur Phys J Spec Top. 2008;153:467-469.
- Wong B, Abrams SH, Sivagurunathan K, et al. In vitro detection of caries beneath dental sealant with the Canary System [ORCA Congress abstract 141]. Caries Res. 2012;46:328.
- Abrams S, Silvertown J, Wong B, et al. Detection of caries around restorations with The Canary System. Poster presented at: IADR General Session; June 22, 2012; Iguaçu Falls, Brazil. Abstract 1824.
- Matvienko A, Mandelis A, Hellen A, et al. Quantitative analysis of incipient mineral loss in hard tissues. Proc SPIE. 2009;7166.
- Hellen A, Mandelis A, Finer Y. Photothermal radiometry and modulated luminescence examination of demineralized and remineralized dental lesions. J Phys Conf Ser. 2010;214:012024.
- Matvienko A, Amaechi BT, Ramalingam K, et al. PTR-LUM-based detection of demineralization and remineralization of human teeth. Presented at: IADR General Session; March 16, 2011; San Diego, CA. Abstract 114.
- Mandelis A, Jeon R, Matvienko A, et al. Dental biothermophotonics: how photothermal methods are winning the race with x-rays for dental caries diagnostic needs of clinical dentistry. Eur Phys J Spec Top. 2008;153:449-454.
Dr. Abrams is a general dental practitioner with more than 30 years of clinical experience. Upon graduation from the University of Toronto Faculty of Dentistry in 1980, he established a group practice in Toronto, Canada, that has grown to involve general dentists and dental specialists. Dr. Abrams is the founder of Four Cell Consulting, Toronto Ontario, Canada, which provides consulting services to dental companies in the area of new product development and promotions. Dr. Abrams founded Quantum Dental Technologies, a company developing laser-based technology for the early detection and ongoing monitoring of dental caries. He is a Fellow of the Pierre Fauchard Academy and the Academy of Dentistry International, American College of Dentistry, a member of the Canadian Academy of Esthetic Dentistry, International Academy of Dento-Facial Esthetics, European Association for Caries Research, and International Association of Dental Research. He has published more than 90 articles in various international publications on topics ranging from early caries detection, prevention, removable prosthetics and restorative dentistry. He has developed the “Triple Laminate Technique” for utilizing soft-tissue undercuts when fabricating complete and partial dentures. In 2002, Dr. Abrams was awarded the Barnabus Day Award from the Ontario Dental Association for 20 years of distinguished service to the dental profession. He is one of the founding board members of ACCERTA Claim Corporations, a dental and pharmacy claims management company. He can be reached at (416) 265-1400 or at dr.abrams4cell@sympatico.ca.
Disclosure: Dr. Abrams is the CEO and cofounder of Quantum Dental Technologies, the maker of the product mentioned in this article.







