

The symptoms of the epidemic of smaller jaws are everywhere. Children are walking around with their mouths open, unable to close them. Adults are snoring. Teenagers are having their misnamed “wisdom” teeth extracted, sometimes with traumatic results. And so many people now have obstructive sleep apnea (OSA) that sterilizers for continuous positive airway pressure machines are being advertised on television.
But the cost, bother, injury, and physical unattractiveness that accompany these symptoms are only the tip of the iceberg. There also is the stress caused by repeated awakenings at night that, in turn, make people more likely to suffer serious insults such as cardiovascular disease, cancer, attention deficit hyperactivity disorder, and perhaps even Alzheimer’s disease. Plus, sleep disturbances result in daytime fatigue that causes poor performance in school and on the job, highway accidents, and possibly injury or death in hospitals where interns may be sleep-deprived.
What’s Behind It All
So why are people increasingly afflicted? The answer is that, especially in industrialized societies, the human jaw is shrinking. It often no longer can comfortably house the tongue, which then slops back and tends to block the airway, causing snoring and OSA. And the cause of that shrinkage is crystal clear. Human cultural evolution has caused a gigantic environmental change as Homo sapiens transitioned from being gatherers and hunters through the agricultural revolution and into the industrial age.
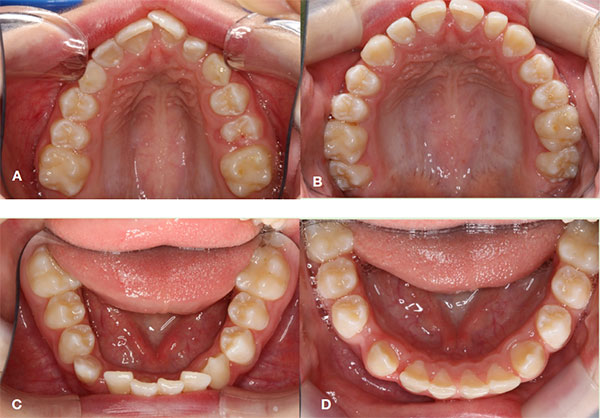 |
| Figure 2: The upper and lower dental arches were typically collapsed with a deep palatal vault and dental crowding (a). The expansion and postural program improved the situation with the face and the dentition (b). But the real health improvement is obvious when the cephalometric radiographs are compared showing a discernable enlargement of the airway. |
For most of humanity’s history, the development of the maxilla and mandible was guided by the gentle pressures of tensions in the jaw muscles applied by the normal posture of the jaws—teeth in light contact, tongue against the palate. But during that environmental transition, the process of jaw development was disrupted by a series of factors, including less breastfeeding, weaning to baby food rather than adult food that requires chewing, an increasingly liquid and “processed” diet, moving indoors where allergens and daycare centers are concentrated (leading often to persistent stuffy noses and mouth-breathing in children), and so on. There’s already good evidence that parental feeding with a spoon is not ideal for the child’s jaw development. Forbidding a five-year-old from chewing gum isn’t ideal either.
Despite the massive evidence that these problems are primarily environmental in origin, we discovered that many dentists still believe that jaw shrinkage is somehow genetic, even citing family resemblance and twin studies in support of that view. It is not necessary to revisit the massive literature on “heritability” demonstrating the fallacies of that approach.
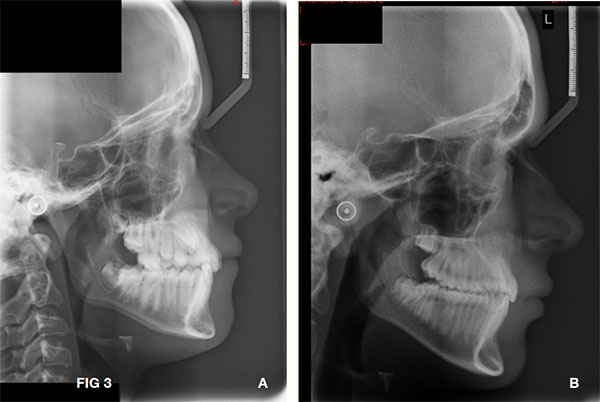 |
| Figure 3: Cephalometric radiographs comparing the size of the airway before (a) and after (b) Forwardontics treatment. |
 |
| Figure 4: See another typical result of another patient of Dr. Simon Wong’s consecutively treated sample, before and after Forwardontics treatment. This clinical work is not unusual in a Forwardontics practice, but the norm. The orthodontic profession should be obsessed with corroborating these clinical results with 3-D full airway scans, polisomnograms, and behavioral and other health markers for these kinds of patients, which are much too common in our society. |
All that is required is to know that jaws have continued to shrink over that past few centuries (say, 20 generations), and there is no evidence that small-jawed individuals are out-reproducing large-jawed individuals are any rate, let alone the high selection pressure that would be required to produce a discernable change in such an eyeblink of evolutionary time. Indeed, if one were to speculate on selection pressures, we think the best guess would be that, considering sleep apnea and the traumas associated with the removal of wisdom teeth, that biological selection pressures would favor larger jaws.
Corrective Care
Perhaps the cheeriest news on the jaws front, particularly for orthodontists, comes from the clinical front.
“Smile Direct within five years will do more orthodontics than all the orthodontists in the United States combined,” said orthodontist Bill Hang, DDS, MSD. “Every practice will be devastated.”
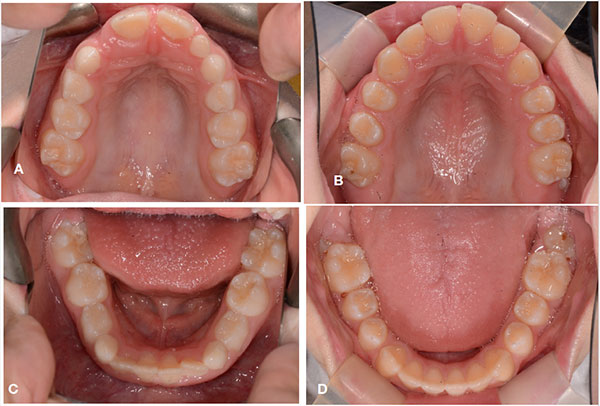 |
| Figure 5: Occlusal results, before (a) and after (b) upper arch, and before (c) and after (d) lower arch. |
 |
| Figure 6: A photographic calibrated superimposition of the before and after treatment, which demonstrated the powerful result of postural and Forwardontics treatment of young patients. |
Orthodontists who primarily move teeth around and create anchors such as retainers to keep them in their new positions will be less in demand. In contrast, those who can prevent m
alocclusion, airway constriction, and long-face syndrome will likely flourish.
The clinical evidence largely generated by Simon Wong, BDSc, indicates that using minimally invasive Forwardontics appliances to train children to keep their mouths shut, accompanied by a carefully designed postural exercise regime such as Good Oral Posture Exercises (GOPex), can return children to the trajectory of normal orofacial development. It also could increase the probability that they will live long, healthy, and happy lives.
A major question for society as a whole is how to supply the needed guidance to those children needing preventive care. It can be a fairly long process requiring dedication on the part of both children and parents and intensive (and often expensive) help from dental professionals.
Those with the skills to oversee an oral posture exercise program are few in number today, which calls for expansion and modification of those delivering orofacial health. It also suggests the need for cultural shifts toward prevention, promoting awareness of oral posture issues, breastfeeding, weaning to solid foods, the importance of “chewability” in diets, prevention of stuffy noses, and so on. All of that is a big order, but success could bring big advantages to future generations.
Dr. Kahn is a graduate of the University of Mexico and the University of the Pacific. She has 25 years of clinical experience in orthodontics and is part of craniofacial anomalies teams at the University of California, San Francisco and Stanford University. She also is the coauthor of Jaws: The Story of a Hidden Epidemic. She can be reached at forwardontics.com.
Dr. Ehrlich has been a household name since the publication of his 1968 bestseller, The Population Bomb. He also is the coauthor of Jaws: The Story of a Hidden Epidemic. He is Bing Professor of Population Studies Emeritus and president of the Center for Conservation Biology at Stanford University. He also is a member of the National Academy of Sciences and a recipient of the Crafoord Prize, the Blue Planet Prize, and numerous other international honors. He investigates a wide range of topics in population biology, ecology, evolution, human ecology, and environmental science. He can be reached at [email protected].
Related Articles
Jaws: The Story of a Hidden Epidemic
Malocclusion, Dental Crowding Appeared Around 12,000 Years Ago
Managing the Rising Trend of Adult Orthodontic Patients



