


INTRODUCTION
Parents are concerned about aesthetics for their children. Aesthetic dentistry can provide a beautiful smile that parents and their children desire. Self image is very important for our young patients so that they can look good and feel good about themselves. We have all experienced that wonderful spontaneous patient smile when we have turned the “ugly duckling” into a “beautiful swan.” We are fortunate to have dental materials and devices that provide us the opportunity to perform aesthetic dentistry. Some of the techniques and materials we have available for our young patients’ smile creations include: porcelain veneers, microabrasion, bleaching, orthodontics (including clear braces and aligners), direct and indirect composite restorations, implants, and all-ceramic crowns.
This article will describe and illustrate various uses of flowable composites that aid in providing aesthetic restorations for children and teens. The advantages of the beauty and functionality will also be elicited.
| Table 1. Indications for Flowable Composites | ||||||||||
|
INDICATIONS FOR FLOWABLE COMPOSITE IN YOUNG PATIENTS
There are many indications for the use of flowable composites in young patients (Table 1). Let’s look in more detail at a few of these.
Preventive Resin Restorations
 |
 |
| Figure 1a. Permanent molar with incipient caries. (Courtesy of Giovanni Olivi) | Figure 1b. Preventive resin restoration. (Courtesy of Giovanni Olivi) |
 |
 |
| Figure 2a. Permanent molar with caries adjacent to failed sealant. (Courtesy of Giovanni Olivi) | Figure 2b. Erbium laser preparation of molar for preventive resin restoration. (Courtesy of Giovanni Olivi) |
 |
 |
| Figure 2c. Preventive resin restoration. (Courtesy of Giovanni Olivi) | Figure 3. Bonded orthodontic brackets. |
Simonsen1 has recommended that, for the type 2 preventive resin restorations (PRR) in which the preparation involves both the enamel and dentin, a flowable composite could be utilized to replace the carious tooth structure after excavation of the incipient caries. In a recent article by Savage, et al2 it was reported that flowable composite was the most widely used restorative material for the PRR among those pediatric dentists surveyed in this study. More than 30% of the pediatric dentists always use a flowable composite or a combination of flowable composite and “packable” composite/flowable composite combination (Figures 1a and 1b).2 The author has found flowable composite to also be useful when a sealant has failed and incipient caries has been detected at a recall visit (Figures 2a to 2c). The Venus Diamond Flow (Heraeus Kulzer) flowable composites offer low shrinkage and high flexural strength.
Bonding Orthodontic Brackets
Vicente and Bravo3 evaluated the shear bond strength of several flowable composites after debonding of orthodontic brackets compared to a traditional orthodontic resin. The shear bond strength was measured with a universal testing machine and the adhesive remnant after debonding was quantified utilizing image analysis. The results showed that there were no significant differences between the shear bond strengths of the various groups evaluated. The orthodontic resin left significantly more adhesive on the tooth than the 3 flowable composites tested.3 Ryou, et al4 in a recent study concluded: “…flowable composites with no intermediate bonding resin could be conveniently applied for orthodontic bonding” (Figure 3).
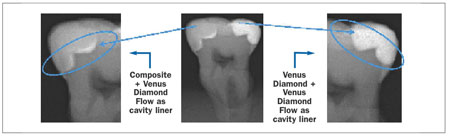
Class II and V Restorations Utilizing Flowable Composite
Flowable composites are often utilized as a liner under composite restorations. The purpose is to seal the margin, which helps prevent postoperative sensitivity and secondary caries. Sadeghi and Lynch5 investigated the effects of a layer of flowable composite and compomer on microleakage of composite restorations that extended apically to the cement-enamel junction. The results of the study showed that when flowable composites were used as a liner, both the packable and the nanofilled composite materials had significantly less microleakage than when flowable liners were not used. There was a significant reduction of the microleakage occurring under both types of composite materials at the gingival floors5 (Figures 4a to 6b).
Illie and Hickel6 investigated the mechanical properties of composites and concluded that flowable composites and compomers showed comparable results. Flowable composites only differed from microfilled composites in diametric tensile strength.
 |
 |
| Figure 4a. Class II preparation on a primary molar. | Figure 4b. Flowable composite placed. |
 |
 |
| Figure 4c. Flowable composite restoration completed. | Figure 5a. Class II preparations of bicuspid and molars. |
 |
 |
| Figure 5b. Flowable composite as a liner. | Figure 5c. Composite placed over flowable composite. |
 |
 |
| Figure 6a. Class V preparation on bicuspid. | Figure 6b. Flowable composite restoration. |
Some of the flowable composites the author uses routinely includes Venus Diamond Flow. The advantages to this particular flowable composite includes the increased strength (versus a sealant), low shrinkage stress, and high flexural strength. It also has the advantage of being an exact shade match with the Venus Diamond composite system. Other flowable composites that the author uses includes GC America’s G-aenial Flo and Universal Flo and Shofu’s Beautifil Flow Plus. The advantage to the later is the release of fluoride. Kerr’s Vertise Flow has the added benefit of being self-etching.
The effects of different light-curing units on the microleakage of flowable composite resins was studied by Yazici, et al.7 They found that none of the Class V restorations restored with flowable composites exhibited marginal leakage of the enamel. Also, there was no significant difference exhibited between the flowable composites tested on the dentin margins.7
Splinting Fractured and Mobile Teeth and Orthodontic Retainers
 |
 |
| Figure 7. Splint bonded with a flowable composite. |
Figure 8a. Fractured permanent central incisor. |
 |
 |
| Figure 8b. Flowable composite bonded fractured segment to crown. | Figure 9. Orthodontic retainer bonded with flowable composite. |
Tabrizi, et al8 found that flowable composites provided satisfactory shear bond strength comparable to a standard orthodontic resin and therefore may be used for direct bonding of lingual retainers.8 Flowable composites may be used to splint mobile teeth utilizing orthodontic wire or nylon filament splints (Ribbond). Foek, et al9 studied the adhesive properties of bonded orthodontic retainers to enamel, utilizing flowable composite, with both stainless steel wire versus fiber-reinforced composites. They found that the bond strengths between the fiber-reinforced composites and the orthodontic wire when used as retainers did not differ significantly (Figures 7 to 9).9
Repairing Small, Direct, and Indirect Restorations
 |
| Figure 10. Occlusal restoration with Venus Bulk Flowable. |
 |
| Figure 11. Radiopacity of a flowable composite material. |
One of the many advantageous properties of flowable composites is their ability to repair previously placed composite restorations. Papacchini, et al10 evaluated the effect of various intermediate resin agents on composite-to-composite bond strengths. The flowable composites showed good interfacial quality to the adhesives. Also, the application of flowable composites resulted in statistically superior tensile strength (Figure 10).10 The author used Venus Diamond Flow in this instance due to the studies indicating its excellent bond strength, low shrinkage stress, and shade matching quality.
| Table 2. The Desirable Properties of Flowable Composite are the Following: | ||||||
|
IMPORTANT PROPERTIES OF FLOWABLE COMPOSITES
Flowable composites exhibit many characteristics that make them an excellent choice for indications like the ones highlighted above (Table 2). The following properties are important when treating young patients with this class of composite resin restorative material.
| Preventive Resin Restorations: Are They Coming of Age? |
|||||||||||||||||||||||
| Tom M. Limoli, Jr With the advent of newer materials and techniques, traditional definitions are frequently misunderstood. A sealant is not a restoration because it involves only the enamel surface of the tooth. The reimbursement for the application of sealants is per tooth, not per surface. Most third-party payers do not consider preventive resin restorations (PRR) to be restorative procedures or reimbursable benefits. They are considered sealant procedures. The academic literature identifies 3 specific types of PRR, while Current Dental Terminology 2011-2012 (CDT), unfortunately, does not. Academically, PRR are classified as either: Type I—utilized when the pit-and-fissure lesion is minimal or when the operator is unsure whether caries is present and does not feel comfortable utilizing simply a pit-and-fissure sealant. The carious tissue is first removed in the most conservative manner possible. If the lesion does not extend into dentin, the tooth is then etched and a pit-and-fissure sealant is applied. Type II—used when caries has progressed into the dentin, yet is still confined to a small area. After caries removal, a protective base of calcium hydroxide can be added to any exposed dentin before the enamel is etched and dentinal bonding agent, unfilled resin, and filled composite resin are applied. A sealant is used for separate pits and fissures on the same tooth. Type III—uses only the filled resin to restore the cavity preparation. Pit-and-fissure sealant is then applied to seal the adjacent fissures. New this year to CDT is procedure code D1352. It is identified as simply “PRR in a moderate to high caries risk patient—permanent tooth.” Its descriptor reads, “Conservative restoration of an active cavitated lesion in a pit or fissure that does not extend into dentin; includes placement of a sealant in any radiating noncarious fissures or pits.” In my opinion, this definition does nothing more than simply identify when a sealant is still a sealant, but can now be somehow classified as being a “super sealant.” So, it is my observation that this CDT procedure code has the potential for healthcare fraud abuse and inappropriate utilization written all over it. Be careful. Never has any form of PRR been appropriately reported with codes D2391. CDT does not specifically address the 3 types of PRR, but it specifically dictate that a restoration is not to be classified as such unless the outline form extends completely into the dentin. If the entire floor of the cavosurface margin is not in dentin, the procedure is to be classified as a sealant with code D1351. |
|||||||||||||||||||||||
|
Radiopacity of Flowable Composites
One of the qualities of a flowable composite that is very favorable is that of being radiopaque. Venus Diamond Flow has been shown to be one of the most radiopaque flowables on the market today. Murchison, et al11 in their study, stated the following: “The level of radiopacity of the tested flowable composites was variable; those with low radiodensity should be avoided in Class II restorations, where a clear determination of recurrent caries by the examining clinician could be compromised.”11 Sabbagh, et al12 agreed with a more recent study when they concluded that flowable composites used within intracoronal restorations, clinicians should use materials with high radiopacity (Figure 11).12
Polishing Flowable Composites
Polishablilty of the surface of the restoration is important for aesthetic and functional purposes. The surface should be able to have a smooth lustrous surface and be able to maintain this desired characteristic. Ozel, et al13 studied the effect of one-step polishing systems on the surface roughness of various flowable composites. The one- or 2-step polishing systems are a good choice for the polishing of flowing composites.13
CONCLUSION
This article briefly described and demonstrated various indications for aesthetic restorations that can be used successfully for our child and adolescent patients. Modern aesthetic techniques and flowable composite resin materials, used properly for purposes such as those presented herein, will serve to broaden the scope of aesthetic dentistry delivered for children and teens.
References
- Simonsen RJ. Preventive resin restorations (II). Quintessence Int Dent Dig. 1978;9:95-102.
- Savage B, McWhorter AG, Kerins CA, et al. Preventive resin restorations: practice and billing patterns of pediatric dentists. Pediatr Dent. 2009;31:210-215.
- Vicente A, Bravo LA. Evaluation of different flowable materials for bonding brackets. Am J Dent. 2009;22:111-114.
- Ryou DB, Park HS, Kim KH, et al. Use of flowable composites for orthodontic bracket bonding. Angle Orthod. 2008;78:1105-1109.
- Sadeghi M, Lynch CD. The effect of flowable materials on the microleakage of Class II composite restorations that extend apical to the cemento-enamel junction. Oper Dent. 2009;34:306-311.
- Ilie N, Hickel R. Investigations on mechanical behaviour of dental composites. Clin Oral Investig. 2009;13:427-438.
- Yazici AR, Celik C, Davangac B, et al. Effects of different light curing units/ modes on the microleakage of flowable composite resins. Eur J Dent. 2008;2:240-246.
- Tabrizi S, Salemis E, Usumez S. Flowable composites for bonding orthodontic retainers. Angle Orthod. 2010;80:195-200.
- Foek DL, Ozcan M, Krebs E, et al. Adhesive properties of bonded orthodontic retainers to enamel: stainless steel wire vs fiber-reinforced composites. J Adhes Dent. 2009;11:381-390.
- Papacchini F, Radovic I, Magni E, et al. Flowable composites as intermediate agents without adhesive application in resin composite repair. Am J Dent. 2008;21:53-58.
- Murchison DF, Charlton DG, Moore WS. Comparative radiopacity of flowable resin composites. Quintessence Int. 1999;30:179-184.
- Sabbagh J, Vreven J, Leloup G. Radiopacity of resin-based materials measured in film radiographs and storage phosphor plate (Digora). Oper Dent. 2004;29:677-684.
- Ozel E, Korkmaz Y, Attar N, et al. Effect of one-step polishing systems on surface roughness of different flowable restorative materials. Dent Mater J. 2008;27:755-764.
Dr. Margolis received his BS and DDS from Ohio State University and his certificate in pediatric dentistry from the University of Illinois College of Dentistry. Dr. Margolis is a clinical instructor at Loyola University’s Oral Health Center and an adjunct clinical assistant professor at the University of Illinois College of Dentistry. He has lectured internationally and has received Mastership from the Academy of Laser Dentistry. Dr. Margolis has contributed articles to both lay and professional journals. He is the author of a book, Beautiful Smiles for Special People, which is a course manual for dental personnel treating the disabled patient. He is co-author of a book, Pediatric Laser Dentistry and Atlas, published by Quintessence. Dr. Margolis is in full-time private practice of pediatric dentistry in Buffalo Grove, Ill. He can be reached at (847) 537-7695 or via e-mail at kidzdr@comcast.net.
Disclosure: Dr. Margolis receives honoraria and products from Biolase Technologies, Inc.








