
Our implant editor, Michael Tischler, DDS, speaks with Scott D. Ganz, DMD, about cutting-edge technology for implant dentistry.
You have been involved with dental implants for many decades as a surgical prosthodontist, contributing to scientific literature and numerous textbook chapters, helping to run live surgical courses, and continuing to be in demand as a lecturer around the globe on a regular basis. What is your motivation?
Dr. Ganz: First, Michael, I want to thank Dentistry Today for the years of dedication to the dental industry in bringing such an array of educational articles from clinicians of all persuasions, specialists and GPs, auxiliaries, and other people from our profession to reach such a wide audience in a wonderful format. I am always honored to have been included in past publications, and in this current edition, as Dentistry Today has always chronicled the progress of modern-day dentistry. On that note, perhaps the publishing industry is one that has also gone through amazing transitions in moving from a fully analog publication into today’s digital world with an online presence. In my humble opinion, the digitization of dentistry has the potential of impacting how most clinicians address the needs of their patients. I say this having been there at the beginning, watching the evolution, and trying to stay one step ahead. The changes that we have witnessed, and are witnessing, provide plenty of motivation for me to continue to push the envelope.
 |
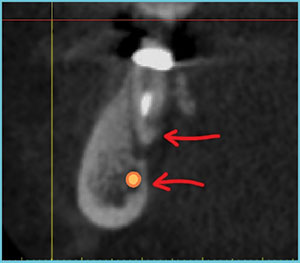
| Figure 1. A reconstructed panoramic image, revealing a periapical radiolucent area surrounding the mandibular right second molar tooth (red arrows). The path of the inferior alveolar nerve (IAN) is shown in orange. (Case submitted by Dr. Barry Kaplan, Morristown, NJ.) |
What do you think of the progress that has been made since you placed your first implant?
Dr. Ganz: As you know, dental implants did not start with Dr. Brånemark. I always like to also give credit to those who risked and invested so much in paving the way to our modern world of dental implants with the blade implant, the subperiosteal implant, pterygoid implants, root form implants in various shapes and sizes, and even today’s zygomatic implants. Pioneers like Greenfield, Strock, Chercheve, Schroeder, Leonard Linkow, Hilt Tatum, Norm Cranin, Jack Hahn, Carl Misch, and so many more set the path for where we are today. So much has changed, and yet there are some things that should remain constant. In fact, some ideas become new again!
What do you mean that “some things should remain constant?”
Dr. Ganz: What should always remain constant is the concept that our patients come to us because they need teeth, not implants. It is our goal to deliver both function and aesthetics, whether for a single tooth or a full-mouth restoration. The foundational conventions of dentistry, such as occlusion, lip support, phonetics, centric relation position, the rule of golden proportions, etc, should be considered for either an analog or a digital workflow. It is my belief that today we finally have the appropriate tools to practice true “restoratively driven” dentistry, with the ability to place implants accurately into restorable positions based upon the needs of the patients and the limitations of the materials that currently exist.
 |
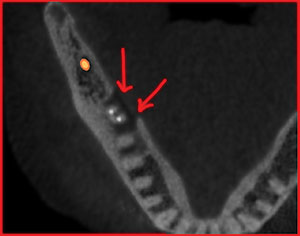 |
| Figure 2. The CBCT scan cross-sectional slice exhibits the path of the IAN in proximity to the molar tooth (lower arrow) and the fenestration of the lingual cortical plate (upper arrow). | Figure 3. The axial view shows the extent of the lesion as it pierces through the lingual cortical plate of the mandible (red arrows). |
 |
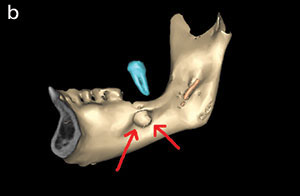 |
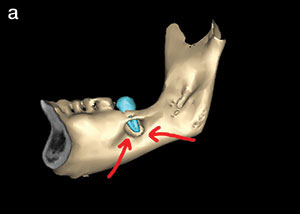
| Figure 4a. Using advanced software segmentation, a 3-D volumetric rendering helps improve the diagnostic phase. The second molar tooth was digitally separated from the mandible (cyan color). | Figure 4b. Having the ability to separate and then move an object like the molar can be an invaluable diagnostic tool. |
 |
 |
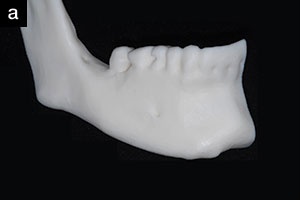
| Figure 5a. The segmented mandible can then be exported as an STL file for 3-D printing of a solid model. The buccal view is seen here. | Figure 5b. The lingual view of the full-scale mandibular model provides excellent visualization of the cortical plate fenestration and position of the molar roots. |
Which tools do you find to be most important? And please clarify how that applies to achieving the goal of restoratively driven dentistry.
Dr. Ganz: This relates back to where we are today, in terms of our progress in the dental industry. We have made great strides in creating implant designs that may have a greater than 95% success rate for more than 20 years. However, we often speak about the success of the osseointegration process and whether implants have been integrated to the bone without a perception of whether or not all the treatment goals were reached—including function and aesthetics. I do not judge success solely on integration, as there is so much more to consider! Although it is nice to say that clinicians are placing implants in the proper restorative positions, even today there are implants placed “where the bone is” and without careful appreciation of the restorative demands. Therefore, I believe that with all of the success that our industry has achieved, the weakest link is still in the first phase of treatment: the diagnosis and treatment planning steps. Therefore, the first most important tool that I will not practice without is computed tomography (CT), or today’s cone beam CT (CBCT). A 3-D image powered by today’s high-powered computers provides the clinician with an interactive environment to assess each patient’s unique and individual anatomical presentation. Michael, both you and I together, and individually, have contributed several articles on this concept within the pages of Dentistry Today and other publica
tions in past years.
 |
| Figure 6. Using an in-house printer with a large enough print bed, it was possible to produce 2 full-scale mandibles, a bone reduction guide, and a surgical drill guide for implant placement (Form 2 [Formlabs]). |
Okay, most clinicians have a clear understanding as to the importance of CBCT in the placement of implants, but what other tools are necessary?
Dr. Ganz: Well, actually, I’m not done with the first part—it’s too important. Even though we have this amazing tool, CBCT, many clinicians still have no real understanding of how to navigate through the software, or how to truly diagnose or treatment plan with or without regard to dental implants. Take, for example, a failing mandibular molar: Can a periapical radiograph reveal the extent of the pathology present? A reconstructed panoramic image reveals a periapical lesion (red arrows) surrounding a lower right second molar tooth (Figure 1). The orange line represents the path of the inferior alveolar nerve (IAN) in close proximity to the lesion. What would be the correct plan of treatment for this case? Do we have enough information from a view similar to a periapical radiograph? What other views would be most helpful?
The CBCT allows for a variety of different views, and each one is important. The cross-sectional view reveals a surprise: The periapical radiolucent area extended significantly through the lingual cortical plate (Figure 2). The upper red arrow points to the lingual aspect of the molar root, and the lower arrow points to the thin layer of cortical bone lingual to the IAN. The axial view shows the extent of the lesion from another perspective. The red arrows clearly show the break in the thick lingual cortical plate (Figure 3). Without 3-D diagnostic imaging, a proper treatment plan would have been, at best, difficult to determine, which could have led to uncontrolled bleeding and, potentially, a sublingual hematoma.
 |
 |
| Figures 7a and 7b. Prior to fabricating a definitive prosthesis, a lab-based tooth design software and CAD application (exocad [exocad GmbH]) prepares a file that can be 3-D printed or milled. |
 |
 |
| Figure 8a. The resin screw-retained mock-up aides in the assessment of fit, occlusion, emergence profile, lip support, midline, and aesthetics prior to the milling of a definitive monolithic zirconia prosthesis. | Figure 8b. The final restoration provides a natural and aesthetic solution for an implant-supported, fixed monolithic prosthesis. |
 |
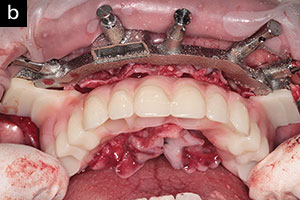 |
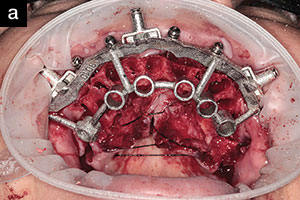
| Figures 9a and 9b. Using advanced 3-D planning concepts, it is possible to provide for tooth extraction, bone reduction, full-template guided implant placement, and abutment connection with a direct connection to a transitional restoration for immediate loading (GuidedSmile Chrome [GuidedSmile Group]). (Images in collaboration with Dr. Isaac Tawil, Brooklyn, NY.) |
 |
| Figure 10. Resonance Frequency Analysis (RFA) technology provides clinicians with a non-invasive, objective method to assess implant stability at the time of placement, at uncovering, or at any time when monitoring the health (integration) of the implant(s) (IDx [Osstell]). |
That is significant! However, you did mention other tools. Can you please elaborate?
Dr. Ganz: Of course! Let’s continue on using this same case example. The first 3 images were taken from the CBCT dataset and represent individual slices in different planes. Many clinicians will still have trouble navigating between these images and may find it difficult to fully appreciate the information at hand. We can then further refine the CBCT data and convert the DICOM data to a 3-D volumetric rendering of the patient’s mandible and teeth through the process of segmentation (Figure 4). Using the density values within the scan data, objects can be created and separated to improve the diagnostic phase. The red arrows clearly point to the large bony lesion within the lingual concavity of the mandible (Figure 4a). The second molar tooth (cyan color) was digitally separated from the mandible based on its density values. These digital tools are becoming invaluable not only in dentistry but also in medicine, simulating anatomical structures and virtual surgical procedures. By separating the virtual molar from the mandible, it can be further manipulated to help determine the best surgical approach (Figure 4b). Finally, the next step in surgical simulation would be to have a physical model of the patient’s mandible in hand to closely examine (Figure 5a).
Advancements in 3-D imaging software allow for the creation of interactive 3-D models, as seen in Figures 4a and 4b. The data utilized for on-screen visualization and manipulation can be converted into STL (standard triangulation language) files for either milling or 3-D printing. The exported STL file of the mandible previously discussed was printed using the process known as stereolithography on an in-office printer (Form 2 [Formlabs]) (Figure 5a). The lateral view reveals the teeth, the mental foramen, and the ascending ramus. There is no evidence of any buccal fenestration, as also evidenced in the cross-sectional image in Figure 2. The lingual view reveals a full-scale representation of the defect as previously described (Figure 5b). The ability to visualize a 3-D printed model can be appreciated by the novice or expert as it represents a physical replica of the patient’s unique anatomy, open for examination.
Scott, that’s a great example of how diagnostic imaging can be used to the maximum. How important do you think in-office 3-D printing is today?
Dr. Ganz: Let’s go back in time for a moment. It was approximately 20 years ago that low-dose CBCT scan devices became available. During the 1990s, and through today, 3-D imaging devices became a major aid in diagnosis and treatment planning for dental implants and a catalyst for the d
evelopment of guided dental implant surgery applications. The majority of surgical guides were fabricated by the process of stereolithography, or 3-D printing on devices that cost hundreds of thousands of dollars. It was a dream to think that, in my lifetime, 3-D printing would become available to the clinician or the dental laboratory technician for the in-house production of surgical guides or biomedical models as seen in Figures 5a and 5b. Three-dimensional printing has become a natural extension of today’s digital workflow—not just from DICOM CBCT data, but also from desktop and intraoral scanners—and an aid for general dental applications; orthodontic aligners; nightguards; crowns and bridgework; digital mock-ups; and much, much more.
By using an in-house printer with a large print bed, it is possible to print 2 mandibles, a bone reduction guide, and a surgical template for implant placement (Figure 6). To evaluate a full-arch monolithic zirconia prosthesis, an STL file is first created by lab-based tooth design software (exocad [exocad GmbH]) and then exported to a 3-D printer (Figure 7). Using a gray-colored resin, the mock-up can be evaluated in the mouth for emergence profile, tooth shape, bite, and lip support to be approved by the patient before the milled restoration is fabricated (Figure 8a). The final monolithic prosthesis can be delivered to the patient with confidence (Figure 8b). The new digital workflow allows for a complete and often seamless communication process between clinician, laboratory, and patient.
Whether they are single-tooth replacements or full-template guidance immediate load complete arches, we as clinicians need confidence that our cases will be successful. Using advanced 3-D planning concepts, we can plan for tooth extraction, bone reduction, implant placement, abutment connections, and transitional prosthetic restorations with a guided or non-guided approach. If true restoratively driven concepts are followed, anatomic landmarks are appreciated, and a partnership is in place with the dental laboratory team (Figure 9).
Is there any other technology that you find indispensable for dental implants today?
Dr. Ganz: Yes, there is. With the amazing diagnostic tools available for planning and placing implants, whether guided or non-guided, we still need information about every implant placed in terms of implant stability and whether an implant is integrated enough to load. While many clinicians believe that insertion torque is a reliable method to determine implant stability, this may be provide a false sense of security. Insertion torque is the frictional resistance of an implant as it is delivered to the osteotomy site at that moment in time, and often it is a subjective measurement. We need an objective, non-destructive measurement that can be documented at the time of implant placement, an hour later, 2 months later, at the time of uncovering, or at any time during the lifespan of the implant. This technology exists as resonance frequency analysis (RFA), which measures implant stability quotient (ISQ). I like the concept of being able to have an entry in the patient’s chart at the time of placement, providing me with critical information relating to when it is appropriate for loading (Figure 10).
Thanks so much for taking some of your valuable time to address some of these important topics related to successfully placing and restoring dental implants. You are a true leader in implant dentistry, Scott!
Dr. Ganz received his specialty certificate in Maxillofacial Prosthetics/Prosthodontics, which led to a focus on the surgical and restorative phases of implant dentistry and to contributing to 15 implant-related textbooks. He is a Fellow of the Academy of Osseointegration, a Diplomate of the International Congress of Oral Implantologists, president of the Digital Dentistry Society, and co-director of Advanced Implant Education. Dr. Ganz is on the faculty of the Rutgers School of Dental Medicine and maintains a private practice in Fort Lee, NJ. He can be reached at [email protected].
Disclosure: Dr. Ganz reports no disclosures.
Related Articles
Treatment Planning for Dental Implants: An Update
Enhanced Diagnosis and Treatment Planning for Implants
Blueprints for Success With Implants

