


INTRODUCTION
Dentists and dental laboratory technicians are well aware of the importance of good communication in order to facilitate the best possible outcomes in restorative cases. Knowing it and doing it, however, are 2 different things, and in many cases there are still a number of gaps in the typical doctor-technician communication process. Whether it is an inadequate impression, or a failure to accurately convey the desired shade, it is not uncommon for dentists to omit helpful information in their instructions to labs. On the laboratory side, some dental technicians may struggle with effectively conveying to dentists how they might communicate this information more clearly.
The increasing expectations of today’s dental patients put additional pressure on the relationships between doctors and their dental technicians. Patients expect a smooth process in the dental office with highly aesthetic results, and they are also expressing a desire for an increased level of comfort during procedures. These factors all contribute to the importance of communication between the dentist and the laboratory.
While any number of factors can contribute to an undesirable result in the restorative process, in many cases “the human element” is likely a major cause. A poor impression or vague instructions on the dentist’s part can start things on the wrong foot, and on the lab side, technique-dependent materials and processes leave a lot to chance. The dental community is discovering that, as in many other industries, reducing some of the human element in the restorative procedure may lead to more predictable and reliable results. At the same time, the technologies used to achieve this goal can also help improve communication between the dentist and the laboratory team.
Capitalizing on Digital Technologies
During the past years, a flood of digital technologies has changed the dental world, many of them offering tools that increase automation and move away from the people-driven techniques that can introduce errors. This is obviously seen in many CAD/CAM technologies and in the newer digital impression-taking systems.
Digital impressions, in particular, can go a long way in improving the team communication between dentists and dental technicians, and in reducing errors. The Lava Chairside Oral Scanner (C.O.S.) (3M ESPE), for example, gives the dentist numerous tools to check and review a digital scan before submitting it to the laboratory, which allows the dentist to ensure that all necessary information has been captured. With digital impression-taking, dentists no longer have to dread receiving calls from their laboratory team with the news that an impression is inadequate; the quality of the impression can be confirmed while the patient is still in the doctor’s chair.
But even with these technologies, the possibility of user error, resulting in restorations being compromised, still exists. One example of this can be seen with certain zirconia crowns. While zirconia itself is known for strength, reports have surfaced in recent years that the porcelain overlays on some of these restorations were prone to chipping. Additional investigation, however, revealed that in most cases, this chipping was due to poor design of the zirconia coping; specifically coping designs that left the overlying porcelain unsupported.1
|
Eliminating Variation
A recently introduced laboratory tool offers the potential to further reduce the chance of this human error in designing zirconia substructures and porcelain overlays; the Lava Digital Veneering System (DVS) (3M ESPE) utilizes a standardized CAD/CAM veneering process to better control the variables in the design of a zirconia restoration. With this system, the zirconia coping and glass ceramic veneer are digitally designed, milled separately, and then bonded together with a special fusion porcelain. The system eliminates the need to hand-layer porcelain, increasing productivity for the laboratory teams and reducing the chance of failure due to improper design.
The Lava DVS is designed to maximize productivity for dental laboratories, but the opportunity also exists for dental technicians to apply advanced techniques to enhance characterization. Each of the 3 components of the system is available in multiple shades and translucencies, and both the zirconia coping and inside surface of the glass ceramic veneer can be customized with multiple shades to produce a highly aesthetic restoration. As with natural teeth, the color comes from within using this system.
This system functions very differently from monolithic restorations, which are popular among many laboratories due to their efficient production, but can only be customized via stain and glaze applied to the exterior of the restorations. The aesthetics of monolithic restorations can be compromised if they are adjusted during the seating and cementation phase. In contrast, with the Lava 3-component DVS, the characterization can be applied internally, thus producing a restoration with translucency and shade variances throughout, creating a lifelike appearance.
Because the Lava DVS utilizes a feldspathic porcelain that is condensed into a block and milled, the variability of this process in the laboratory is dramatically reduced. Research2 has shown the variability among ceramists in this process—no 2 ceramists condense at the same density, even on the same day. Even ceramists at high-end laboratories may not be skilled at properly condensing porcelain. With porcelain condensed in an automated process, dental technicians can be assured that there are no imperfections. In turn, this consistency adds to the strength of the restoration. The quality of the laboratory’s product is consistent between technicians and their various levels of experience. Due to the strength2 of these restorations, they are indicated for patients requiring a posterior full-coverage option. The results of one study that compared the strengths of CAD/CAM sintered to zirconia to both hand veneered and pressed to zirconia copings produced significant findings; the strength of the CAD/CAM sintered restorations was about 80% stronger than when using the other fabrication techniques.2 The following case will demonstrate the use of the Lava DVS system to produce an aesthetic posterior crown, highlighting the simplified communication between the dentist and the dental laboratory team.
CASE REPORT
Diagnosis and Treatment Planning
A patient presented to the office with a fractured buccal cusp on tooth No. 3 (Figure 1). The tooth had originally been restored with a direct filling restoration, followed by a composite inlay when the original restoration failed.
Due to the amount and location of missing tooth structure after this latest break, it was determined that a full-coverage crown would be the best method of treatment.
Preparation Appointment
The tooth was prepped, and a digital scan was captured (Lava C.O.S.) (Figure 2). After scanning the prep and the opposing arch, and reviewing the scan for completion, the case was submitted to the dental laboratory. Photographs, along with a desired shade for the restoration, were also captured to share with the dental laboratory team. A provisional was fabricated using a bis-acrylic material (Protemp Plus [3M ESPE]) and cemented with a provisional cement (Temp Bond Clear (resin) [Kerr]). After checking the occlusion and confirming a balanced bite, the patient was dismissed.
Dental Laboratory Technical Protocol
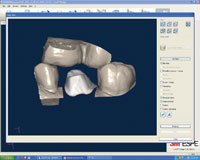
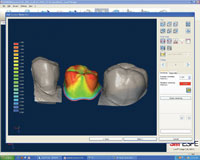
At the dental laboratory, the Lava Scan ST Design System (3M ESPE) was used to review the scan (Figure 3). The software was used to electronically mark the margins and cut the die, and the digital impression was sent to the Lava C.O.S. model production facility. Concurrently, the laboratory team utilized the software to design the porcelain overlay. Using the data captured in the digital scan, the software designed the crown from the outside in to provide maximum strength (Figure 4). The software indicates with a color scale how thick the overlay material is, and alerts the technician if the thickness is beyond acceptable levels (Figure 5).
 |
 |
| Figure 1. Patient presented with a fractured buccal cusp on tooth No. 3. | Figure 2. The prepped tooth, prior to scanning (Lava C.O.S. [3M ESPE]). |
 |
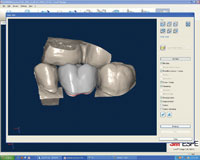 |
| Figure 3. The digital scan submitted by the dentist with margins marked. | Figure 4. The software generated the finished crown from the outside in. Once the full-contour restoration was designed, the software cut the design into segments for the zirconia coping and glass ceramic veneer. |
 |
 |
| Figure 5. The color-coded design of the zirconia core informs the user where overlay material may be too thick. | Figure 6. A very thin layer of fusion porcelain was applied to the coping and fired. |
The design was completed and the zirconia coping and glass ceramic veneer components were milled separately in the Lava CNC 500 Milling Machine (3M ESPE).
After the coping was milled, a thin layer of fusion porcelain was applied and the coping was fired to set the color (Figure 6). (This is an optional step in the Lava DVS process, performed in this case to add advanced characterization.) Once the stereolithography model reached the laboratory, the coping was tried on the model to confirm its fit. To fuse the components together, the Lava DVS veneer was placed in water for one minute to allow the water to infiltrate the veneer. Lava DVS fusion powder and modeling liquid were then mixed in a 1:1 ratio and the resulting fusion porcelain was applied to the inside of the veneer, as well as to the occlusal side of the zirconia coping (Figures 7 and 8). The veneer was then seated onto the coping, and the combined pieces were placed on a tissue to allow excess fusion porcelain to be absorbed. Minor corrections were made to the cervical areas with Lava DVS fusion porcelain and the restoration was removed from the die. The crown was then fired on the fusion firing cycle (Figure 9). After firing, the proximal and occlusal contacts were again checked on the die (Figures 10 and 11). Buccal and lingual areas were fine tuned, and occlusal fissures were adjusted. Staining and glazing was then performed, followed by a final firing (Figure 12). The restoration was then returned to the dental office.
Seating Appointment
Once at the office, the crown was tried in for fit and aesthetics. The crown was then cemented using a self-adhesive composite resin cement (RelyX Unicem [3M ESPE]). The dental team and patient were very happy with the fit and aesthetics; and final photos were captured and the patient was dismissed. The restoration is shown in Figure 13 at 5 months postoperatively. It exhibited good function, excellent aesthetics due to customization of the overlying porcelain (after milling and fusion), and the soft tissue was healthy and well-adapted (Figure 13).
 |
 |
| Figure 7. The zirconia coping, glass ceramic veneer, and fusion powder. | Figure 8. The fusion powder was mixed with modeling liquid, and then applied to both the occlusal surface of the coping and the interior of the veneer. |
 |
 |
| Figure 9. The coping shown here, after the components were fired together. | Figure 10. The coping fit precisely on the die after firing. |
 |
 |
| Figure 11. The die was seated back into the model, demonstrating excellent fit and ample contacts between the mesial and distal surfaces. |
Figure 12. The occlusion was adjusted and color was applied to occlusal surfaces. |
 |
| Figure 13. Restoration shown 5 months after cementation. |
CLOSING COMMENTS
The smoothly executed team procedure demonstrated here is typical of restorations fabricated with the new digital tools currently available. Because the restoration was produced digitally from beginning to end, the opportunity for errors to be introduced was minimized, and the restoration fit very well both on the model and in the patient’s mouth. The Lava DVS is designed to offer excellent aesthetics via characterization, without a significant time investment by the dental technician. At the same time, the digital tools used in the case facilitated communication between the dentist and lab, providing clear directions and information.
Many dentists wish that they could have a laboratory technician working alongside them; digital technology is a means to that end. It helps in making the flow of information between the clinical and dental laboratory teams seamless and efficient, as if they were working side by side. In addition, the introduction of digital technologies actually serves to simplify dialogue, rather than complicating matters.
Every clinician who practices restorative dentistry faces the challenge of delivering work that provides long-term function and is consistent in quality, fit, and aesthetics; and dental laboratory teams must also continually strive to provide outstanding technical solutions. By working as a team, and utilizing digital tools designed to facilitate collaboration, dentists and dental technicians can provide patients with the best in restorative outcomes.
References
- Komine F, Blatz MB, Matsumura H. Current status of zirconia-based fixed restorations. J Oral Sci. 2010;52:531-539.
- Beuer F, Schweiger J, Eichberger M, et al. High strength CAD/CAM fabrication veneering material sintered to zirconia copings – A new fabrication mode for all-ceramic restoration. Dent Mater. 2009;25:121-128 [Epub July 11, 2008].
Dr. Ringer is a graduate of the University of the Witwatersrand Dental School in Johannesburg, South Africa, and completed a mini-residency program at the University of California, Los Angeles. He received his California dental license in 1979. Dr. Ringer is a member of ADA, California Dental Association, and Orange County Dental Society; an accredited member and board member of American Academy of Cosmetic Dentistry; and the founder and president of Orange County Academy of Cosmetic Dentistry. He is a faculty mentor at Spear Education in Scottsdale, Ariz. During the last 18 years, Dr. Ringer has divided his time among treating private patients, teaching at local dental institutions, and speaking at various dental meetings. He can be reached at drringer@dentalcosmetics.com.
Disclosure: Dr. Ringer reports no disclosures.
Mr. Okon holds a bachelor of science degree in microbiology from University of California in Los Angeles (UCLA) and a degree in dental technology from Pasadena City College. He currently serves as president of the Dental Lab Owners’ Association of California for the 2011-2012 term. He is the principal of Stanley Okon Dental Laboratory, Inc, in Orange County, Calif. Mr. Okon is currently a beta tester for 3M ESPE new products and has completed product evaluations for clinical research. He is also participating with UCLA in a new product research study. Mr. Okon is a member and the preferred lab of the Orange County Chapter of the Seattle Study Club and is involved with several other implant study clubs as well. Mr. Okon has lectured for major dental manufacturers, including 3M ESPE, Straumann, Vita, Zimmer, and others. He can be reached at stan.okon@okonlab.com.
Disclosure: Mr. Okon reports no disclosures.





