


INTRODUCTION
Transitioning from a terminal dentition to complete dentures can be an aesthetic and functional challenge. Immediate complete dentures (ICDs) are prosthetics that are inserted at the time of extraction. They can serve a crucial role, as they allow patients to maintain prosthetics throughout their transition to edentulism. They can offer many other benefits to patients, including soft-tissue support, maintenance of vertical dimension of occlusion, and more predictable healing of the ridges and soft tissue.1-3
Immediate complete dentures are not without their disadvantages; unlike conventional complete denture workflows, clinicians cannot complete a full clinical try-in. This leads to unpredictability, not only in anterior aesthetics but also in function. Without this step, it is difficult to communicate what wearing a denture will feel like or if the patient can even tolerate the sensation on the palate. Additionally, establishing centric relation position can be particularly challenging in the presence of a mobile, painful, or otherwise compromised terminal dentition.
There are 2 categories of immediate dentures: (1) classic immediate dentures (D5130/D5140), which are intended to serve as a long-term definitive restoration, and (2) interim immediate dentures (D5810/D5811), which are intended to be replaced after healing. The greatest benefit of classic immediate dentures is the cost to the patient. Although these are typically done for a higher fee than other types of complete dentures, the patient is only responsible for the cost of one set of dentures. With interim immediate dentures, the initial cost is lower, but the patient will pay for a second set of conventional dentures (or implant overdentures) after healing. This allows the clinician to make changes to the tooth arrangement in the definitive set, improving aesthetics and function.3 No matter the type of prosthesis chosen, digital dentistry can help increase the predictability of immediate complete dentures and shorten the workflow.
While ICDs were first introduced in the literature in the 1930s,2 the protocol remained very similar until the advent of digital dentures in the 2010s. There is now widespread use of intraoral scanning for immediate and other complete dentures.4 A decade after the commercial availability of digital dentures,5 there are now numerous case reports incorporating scanning into ICD workflows.6-9 The following case report walks through a fully digital workflow to fabricate an immediate complete denture.
CASE REPORT
An 83-year-old, long-term patient of the practice had been maintaining her dentition through routine periodontal maintenance and with a transitional removable partial denture (RPD) (Figure 1). She presented to an emergency appointment with a chief concern of pain in her upper left molars. After a clinical exam including endodontic testing, it was determined that both of her upper left molars would require root canal therapy. Due to canal calcification, the result would be unpredictable. She was not interested in proceeding with that plan and requested extraction. She was advised that with extraction of the 2 painful teeth, her remaining maxillary dentition could no longer predictably support an RPD as she carried a diagnosis of periodontitis in her maxillary dentition (stage 3, grade B) concurrent with diabetes and traumatic occlusion due to loss of posterior support. She had Class II mobility on her remaining maxillary anterior teeth and Class I mobility on her maxillary molars. After inviting and answering questions, the patient was eager to proceed with an interim immediate complete denture, followed by the fabrication of a definitive complete denture.

Figure 1. The patient presented with irreversible pulpitis on teeth Nos. 14 and 15. Endo prognosis was poor, and the patient did not want to proceed with the procedure. Due to lack of remaining stable abutment teeth, an interim immediate complete maxillary denture was treatment planned.
The patient was very aesthetics-focused and requested that the shape and size of the anterior teeth of her interim immediate denture resemble her current dentition. To more predictably achieve this goal, a digital workflow was chosen. Due to her reduced periodontium, odontogenic pain, and the mobility of her maxillary teeth, an intraoral scan was used for the final impression.
A complete denture design using the denture module on the 3Shape Dental System (3Shape) was used, morphing the anterior design to follow the patient’s existing teeth. Bilateral balanced occlusion was designed in excursive movements in the software (Figure 2). The teeth were nested in segments and fabricated along with the base using additive manufacturing (carbon M3) with denture tooth and base resins (Lucitone Digital Print Denture System [Denstply Sirona]). The teeth were fused to the base, and the prosthesis was finished and polished.
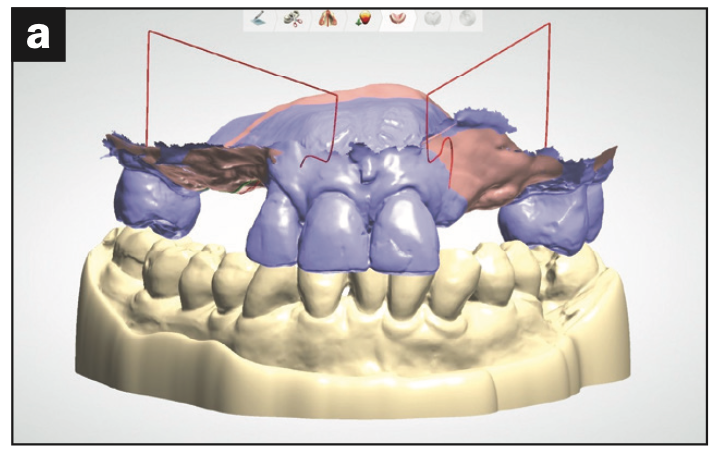
Figure 2a. The patient’s pretreatment scan was loaded into the design software.
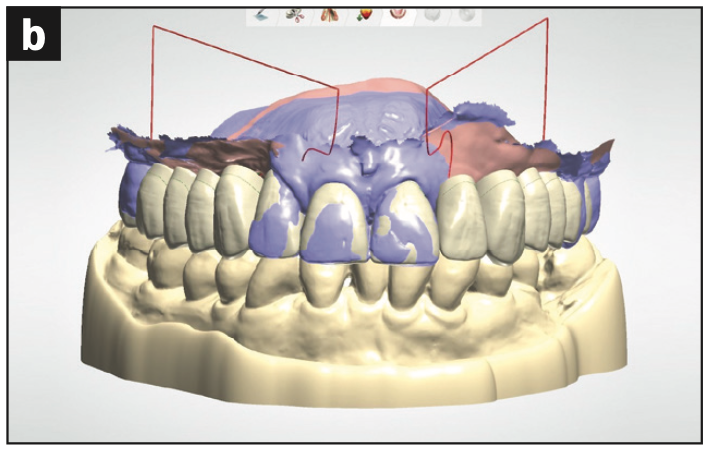
Figure 2b. A tooth mold was chosen from the 3Shape library that closely matched the patient’s existing centrals, and the teeth were morphed to match more closely.
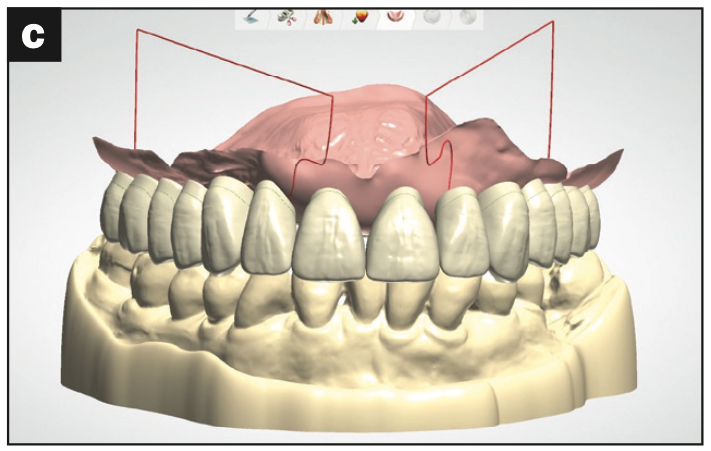
Figure 2c. The complete immediate den- ture arrangement was finalized based on the opposing dentition.
Care was coordinated with an oral maxillofacial surgeon, who extracted the remaining maxillary dentition with local anesthesia. At the completion of extractions, the denture was relieved of high spots and relined with a chairside soft reline material (COE-SOFT [GC America]), and occlusion was adjusted for bilateral balance (Figure 3). This prosthesis was worn and maintained with chairside reline (COE-SOFT) for approximately 6 months following standard protocol (Figure 4).

Figure 3. The immediate complete denture at the time of insertion.

Figure 4. The prosthesis was maintained with chairside soft reline for about 6 months.
At a follow-up appointment, the requested changes were discussed with the patient. Vertical dimension of occlusion and bilateral balanced occlusion were verified. The patient was happy overall with aesthetics but wanted a slightly bolder and larger mold. The midline was also adjusted. The changes were minimal, and though the monolithic try-in could have been skipped, the patient preferred a try-in before proceeding with the final prosthetics.
The soft reline had been well-adapted and contoured, with the prosthesis having excellent support, stability, and retention. Subsequently, a reference denture workflow followed, scanning the prosthesis (intaglio and teeth), along with the opposing dentition, and a centric relation scan was also taken (Figure 5). These were uploaded into design software, and changes were incorporated before printing the monolithic trial denture (Figure 6).
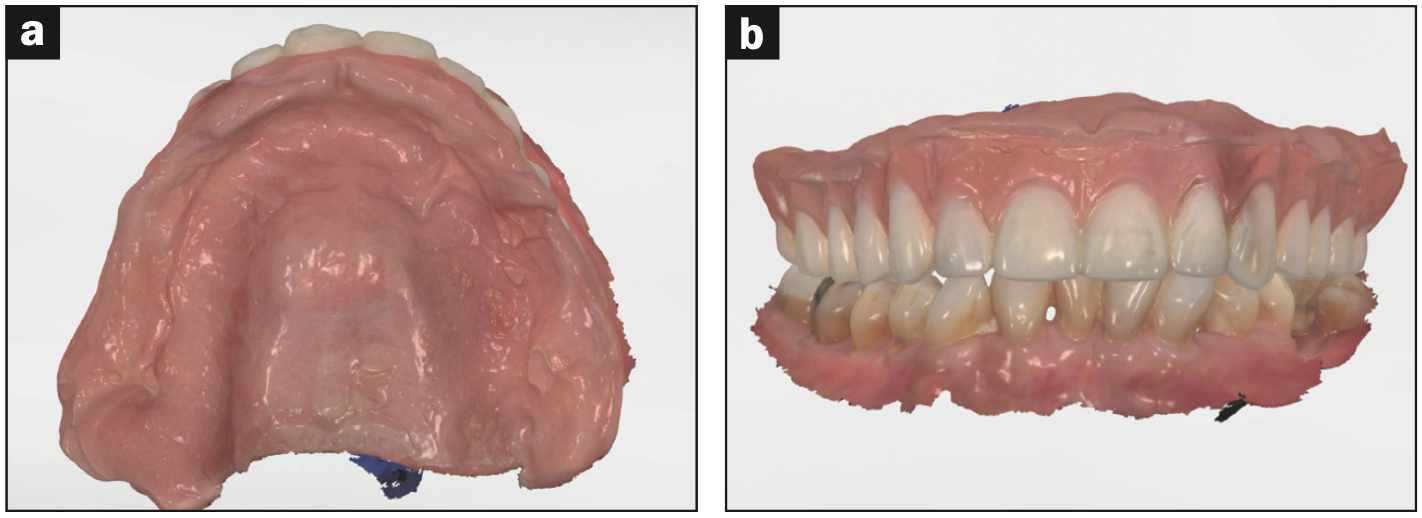
Figure 5. The prosthesis was scanned, along with the opposing dentition and interocclu- sal record, so that the laboratory could follow a reference denture workflow.
At the try-in, the clinician and patient walked through the checklist together (Appendix 1), and no changes were needed. The try-in was printed in an FDA-cleared resin (Lucitone Digital Value [Dentsply Sirona]), and the patient was sent home with the trial denture to identify any sore spots prior to the insertion visit. The definitive dentures were fabricated with the same materials and method as the ICDs.
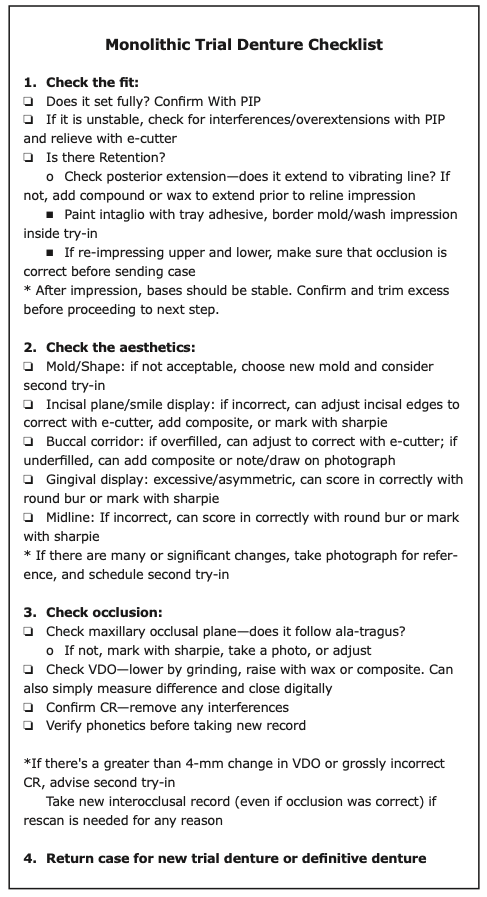
Appendix 1
The dentures were inserted and adjusted following conventional protocols (Figures 6 and 7).

Figure 6. The monolithic printed try-in was completed to verify changes in fit and aesthetics.
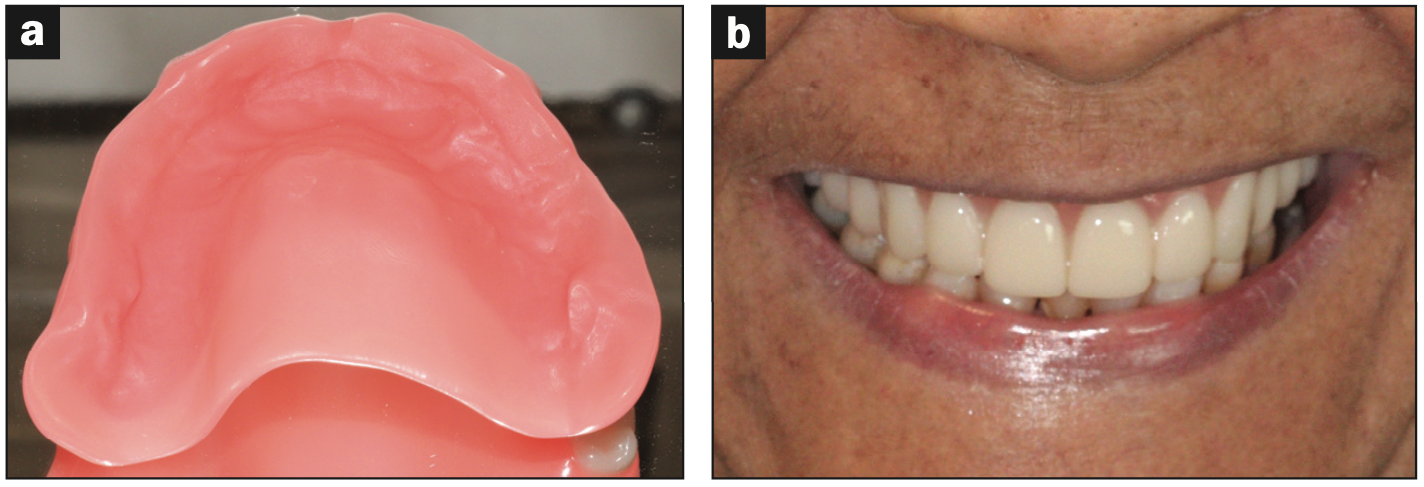
Figure 7. Final prosthesis after healing.
DISCUSSION
Immediate dentures serve a role in preserving function and quality of life after extraction. One must consider, though, they are not without their disadvantages. Literature and clinical experience from providers corroborate the narrative that immediate complete dentures are a consistent challenge. After working with numerous students and clinicians over the years, one of the biggest frustrations with complete dentures in general is the lack of predictability. There is so much room for error along the often long and tumultuous process that it can prove to be frustrating to both clinicians and patients. Following conventional denture workflows, records are destroyed; a remake or modification often requires going back several steps to regain traction. Immediate denture workflows amplify this challenge. The unpredictability is greater due to lack of try-in, and going back to pre-extraction records is virtually unachievable.
CAD/CAM dentures overcome some of these challenges. The preservation of records is often an underappreciated aspect of the workflow. By merging files and photos and customizing molds for the patient, we can now achieve results that would be impossible through conventional workflows. Clinicians can go back to a previous try-in or remake a denture without any additional clinical steps. In other words, the process is more predictable—and less stressful.
Often, the monolithic try-in has a steep learning curve for clinicians new to digital dentures. Included here is a checklist that has helped my students and me through the learning process (Appendix 2). This monolithic trial denture can be quite versatile. It may be partially printed for immediate dentures. If printed in an FDA-cleared resin, it may be worn as an interim denture or worn home short- or long-term for the patient and family to evaluate function and aesthetics. It can then be maintained by the patient as a “backup denture” if something were to happen to his or her prosthesis.
CLOSING COMMENTS
Historically, classic (or conventional) immediate dentures were more common, using the immediate denture as a definitive prosthesis. In this workflow, typically, posterior teeth were removed and custom impression trays were made after healing, then conventional border molding, records, and posterior tooth try-ins were completed before processing. While this achieved the best possible result, unpredictable surgical healing, lack of a try-in, and patient factors remained a challenge. With the ability to duplicate and preserve records, perhaps a paradigm shift toward interim immediate dentures should be considered. Overall, the workflow presented (interim immediate followed by reference/copy denture) should typically result in fewer clinical appointments and less chair time than the conventional/classic immediate denture workflow (Appendix 2).
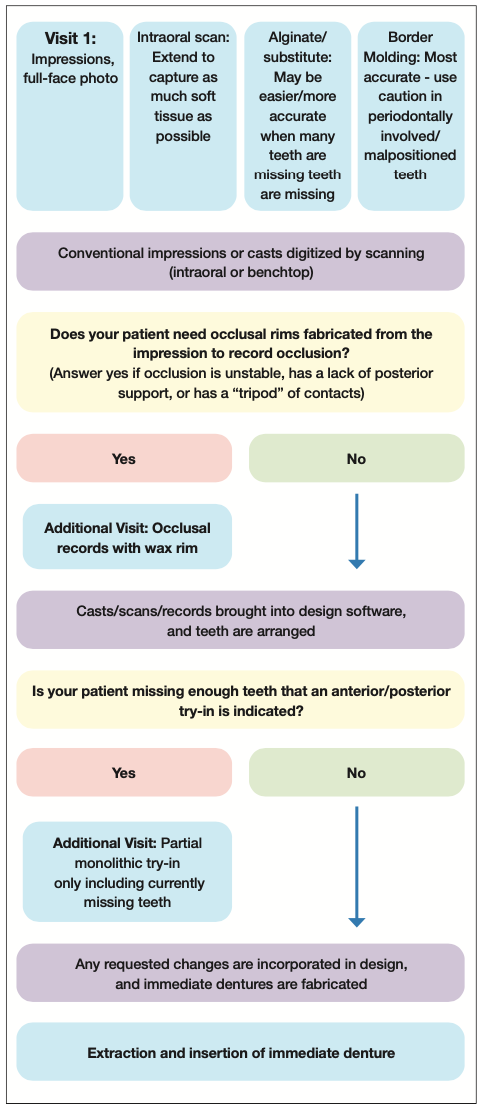
Appendix 2. Proposed digital immediate complete denture workflow.
Another benefit of digital dentistry in the immediate denture workflow is the ability to scan the final impression. When patients are missing many teeth, particularly in the posterior mandible, the soft-tissue scan can be a challenge, and a conventional impression is often the best choice. When many teeth are remaining, however, intraoral scanning becomes much easier.
To summarize, there is not one correct workflow for complete dentures. CAD/CAM offers clinicians numerous ways to improve the complete denture workflow and customize it to work for their practices.
REFERENCES
1. Kelly EK, Sievers RF. The influence of immediate dentures on tissue healing and alveolar ridge form. J Prosthet Dent. 1959;9(5):738–42.
2. Seals RR Jr, Kuebker WA, Stewart KL. Immediate complete dentures. Dent Clin North Am. 1996;40(1):151–67.
3. Rahn AO, Ivanhoe JR, Plummer KD. Textbook of Complete Dentures. 6th ed. Shelton,CT: People’s Medical Publishing House; 2009.
4. AlRumaih HS. Clinical applications of intraoral scanning in removable prosthodontics: a literature review. J Prosthodont. 2021;30(9):747–62. doi:10.1111/jopr.13395
5. Goodacre CJ, Garbacea A, Naylor WP, et al. CAD/CAM fabricated complete dentures: concepts and clinical methods of obtaining required morphological data. J Prosthet Dent. 2012;107(1):34-46. doi:10.1016/S0022-3913(12)60015-8
6. Mendonça G, Edwards SP, Mayers CA, et al. Digital immediate complete denture for a patient with rhabdomyosarcoma: a clinical report. J Prosthodont. 2021;30(3):196-201. doi:10.1111/jopr.13305
7. Neumeier TT, Neumeier H. Digital immediate dentures treatment: a clinical report of two patients. J Prosthet Dent. 2016;116(3):314–9. doi:10.1016/j.prosdent.2016.01.010
8. Fang JH, An X, Jeong SM, et al. Digital immediate denture: a clinical report. J Prosthet Dent. 2018;119(5):698-701. doi:10.1016/j.prosdent.2017.06.004
9. Clark WA, Duqum ID. Dentsply Sirona: Lucitone Digital Print Denture. LMT Communications. 2021.
ABOUT THE AUTHOR
Dr. Clark completed her doctoral degree from the Marquette University School of Dentistry in Milwaukee and earned her master’s degree in clinical dentistry and certificate in postgraduate prosthodontics from the University of Alabama at Birmingham School of Dentistry. She practiced prosthodontics for 7 years with Team Atlanta (Goldstein, Garber, and Salama), before her current full-time prosthodontic faculty role in at the University of North Carolina Adams School of Dentistry. She has been named a “Leader in Continuing Education” by Dentistry Today for the last 6 years, presenting on a wide range of prosthodontic topics. She recently received the young alumna of the year award from the Marquette University School of Dentistry and the Hunt Memorial Teaching Award from the University of North Carolina Adams School of Dentistry. She has published articles in numerous peer-reviewed journals and serves as a key opinion leader for multiple companies on digital dentures. She can be reached at wendyauclair@gmail.com.
Disclosure: Dr. Clark serves as a KOL for Avadent Digital Dentures and Dentsply Sirona, but she received no compensation for writing this article.








