

A patient came in with severe pain in the upper right quadrant. She had gone to urgent care, which gave her antibiotics because they thought she had a sinus infection. The pain got better for a week but came back. She then went to her dentist, and he did not see anything.
After she found me on social media with my “SHORT Case of the Day,” she came to my office for a consult. The periapical radiograph did not show any obvious pathology. Tooth No. 3 had a previously treated root canal with a post and a crown (Figure 1). Tooth No. 4 was pulp-tested normal.
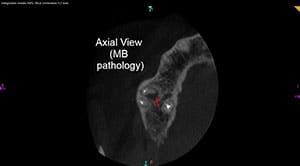
I took a large-field-of-view CBCT using a Carestream CS 8100 (Figure 2). The axial view showed pathology associated with the mesiobuccal (MB) root and a missed second mesiobuccal canal (MB2) (Figure 3). The coronal view showed pathology where the MB2 would exit (Figure 4). The sagittal view showed pathology associated with the MB root (Figure 5). However, the coronal view of the palatal root showed no pathology (Figure 6). The distobuccal (DB) root was short, but there was no pathology there as well.
 |
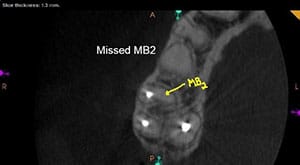 |
| Figure 2. A Carestream CS 8100 provided a large field of view CBCT scan. | Figure 3. There was a pathology associated with the MB root and a missed MB2. |
 |
 |
| Figure 4. The coronal view revealed pathology where the MB2 would exit | Figure 5. The sagittal view showed pathology associated with the MB root. |
 |
 |
| Figure 6. The coronal view of the palatal root showed no pathology. | Figure 7. The patient was asymptomatic during the follow-up visit. |
I retreated tooth No 3. I also located and treated an MB2. It had a single portal of exit. The MB2 is there 90% of the time and has a single port of exit 40% of the time on maxillary first molars. I retreated the MB and DB roots as well. I did not retreat the palatal root due to the large post, and there was no pathology. Removing this post could further weaken the tooth.
The patient returned for a follow-up completely asymptomatic (Figure 7). The CBCT allowed me to visualize the source of the pathology as well as which root the pathology was located in, while helping me avoid unnecessary treatment on the palatal root.
Dr. Short attended the Medical College of Georgia School of Dentistry to attain a DMD degree in 1999. In 2002, he earned his post-doctorate degree in endodontics from Nova Southeastern University and then became a Diplomate of the American Board of Endodontics in 2009. Dr. Short is an expert consultant in endodontics to the Georgia Board of Dentistry, author, speaker, and assistant clinical professor at the Dental College of Georgia in Augusta. His private practice, Apex Endodontics PC, is located in Smryna, Ga. He can be reached at [email protected].
Related Articles
A Short Case Study: Large Cyst or Granuloma?
A Short Case Study: Everything Including the Kitchen Sink!
A Short Case Study: Separated Instruments? Perforation? Relax!



