


The all-ceramic restoration market, including that for zirconia, lithium disilicate, and lithium silicate, has been growing rapidly worldwide since the beginning of the 2000s. With the increasing market demand, various dental manufacturers market different dental ceramics that can be used in many dental prosthetic applications. These materials require different minimum thicknesses and preparations to successfully function in the oral environment.
STRENGTH OF DENTAL CERAMICS (FLEXURAL STRENGTH)
The most common method of measuring ceramic strength is by evaluating its flexural strength (in megapascals). The flexural strength test applies a force on the top of a ceramic specimen, which causes the specimen to bend and fracture. The International Standards Organization (ISO) and the ADA have developed a standard for measuring the flexural strength of dental ceramics. Two methodologies are commonly used today:
l The biaxial flexural strength method (Figure 1)—a circular, ceramic specimen/disc is supported by 3 points, and force is applied in the middle.
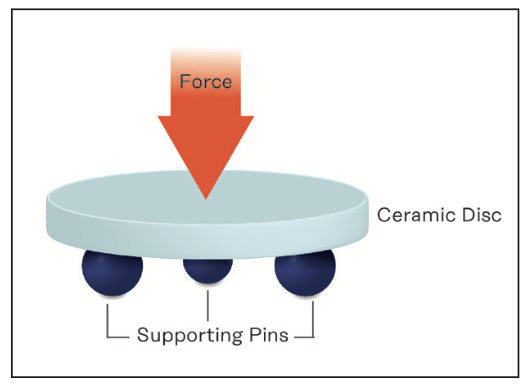
Figure 1. Two-point bending flexural strength test.
l The 3-point bend method (Figure 2a)—a rectangular specimen/bar is used and supported by 2 points, and force is applied in the middle. The 3-point bending test for flexural strength is mostly used with zirconia.
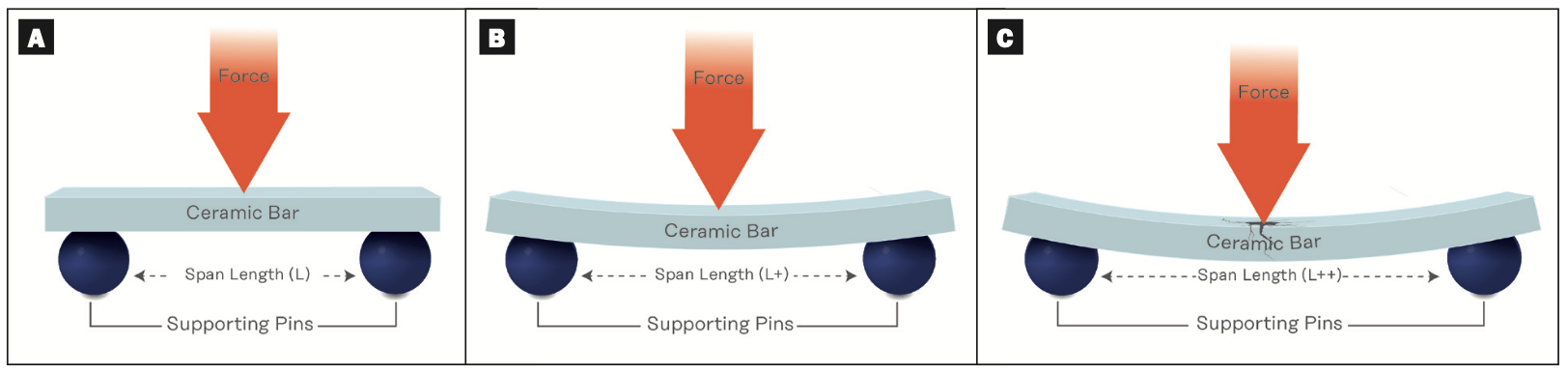
Figure 2. Three-point bending flexural strength test with different span lengths.
Both tests are acceptable; however, ceramics tend to produce higher values when tested with the biaxial method compared to the 3-point bend method.
Furthermore, even in a 3-point bending test, if the span lengths (Figures 2b and 2c) of the specimens are increased, ceramic tends to bend abruptly and fail or crack easily. The span-length setting in the 3-point bending test for flexural strength plays a critical role in establishing the flexural strength test value.
The ISO does provide a guidance on testing that ceramic bars can be in the span length of 12 to 30 mm, but 12 mm and 30 mm can produce completely different flexural strengths; in other words, the shorter the span length, the higher the flexural strength. It is important that clinicians and dental ceramists understand the testing conditions before comparing or selecting the best ceramic for suitable clinical conditions.
INCREASING THE STRENGTH OF CERAMICS
The most straightforward method of increasing the strength of a ceramic is to increase its thickness. This means the preparation depth needs to be higher and may not be favorable in a minimal intervention. There are times when the clinical situation itself may limit the thickness to which a tooth can be prepared (eg, with lower incisors). In these cases, another option is to select a stronger ceramic material. In general, dental zirconia has a higher strength compared to lithium disilicate.
Another option is to adhesively (resin) bond the ceramic restoration to the tooth surface. This will easily increase the fracture resistance of a ceramic.
Kuraray Noritake has a legacy of inventing groundbreaking technologies in resins and ceramics. We invented and introduced the MDP monomer in 1981. All Kuraray Noritake PANAVIA cement brands (Figure 3) contain this original MDP monomer. These cements perform best with KATANA Zirconia material (Kuraray Noritake) (Figure 4).
Figure 3. PANAVIA SA Cement Universal Resin Cement (Kuraray Noritake).

Figure 4. KATANA Zirconia HTML Plus (Kuraray Noritake).
Currently, due to the wide availability of different materials, it is important to understand and properly interpret ceramic strength before comparing or selecting material for clinical use.
For more information, call Kuraray America at (800) 879-1676 or visit kuraraydental.com.








