
One of the most difficult aspects for the clinician in doing root canal treatment is gaining access in patients who have limited mouth openings or small mouths. Common scenarios include treatments in children and the elderly or patients with trismus due to space infections or temporomandibular joint disorders. Nonetheless, if root canal treatment is indicated, one must find a way to perform it, no matter the clinical limitations.
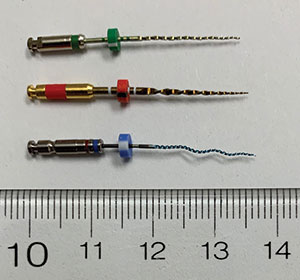
This article will discuss various clinical tips and tricks that will help clinicians in the above scenarios. Various endodontic instruments that are currently available and recommended for use in patients who have limited mouth openings will also be discussed (Figure 1).
Small Hand Mirror
Visibility in endodontics is essential. For instance, one cannot do proper and efficient root canal treatments without the ability to see the occlusal surface of the tooth during access preparation or inside the endodontic access. For nearly all teeth, direct vision will not suffice, as the opposing arch obstructs one’s view. And, once the tooth is endodontically accessed, it is imperative that the clinician be able to directly visualize the pulp floor and locate the canals. In turn, the use of a hand mirror is required; however, many clinicians tend to use a standard size 5 mirror, which is quite large and unnecessary. This could be an issue in patients with limited openings and when a handpiece or fingers holding files take up space over the tooth. As such, a size 3 mirror would be small enough to gain access into small mouths and sites with limited openings while being large enough to see everything needed for carrying out root canal treatment. In Figures 2 to 5, you can see how a smaller size 3 (Integra Miltex Instruments, USA) mirror can be more easily positioned to allow visualization vs an unnecessary and larger size 5 mirror.
 |
| Figure 1. A pediatric patient with small mouth openings. |
 |
 |
| Figure 2. Note size 3 and 5 (left) mirrors alongside a quarter coin. | Figure 3. Access for visibility into a small space was facilitated with a small/size 3 hand mirror. |
Hold Hand Files at 90°
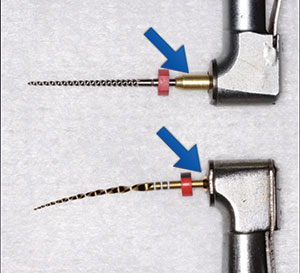
Proper handling of a stainless steel hand file is one of the most important tips for facilitating access. Many clinicians hold hand files with the file directed somewhat along the axis of their fingers (index and thumb). Doing so makes it almost impossible to gain access when the opposing arch is in the way and there is a limited mouth opening. Instead, one should hold the hand file at approximately 90° to the direction of his or her fingers. This should be considered in just the same way as any endodontic handpiece that holds a NiTi motorized file at 90° to the shaft of the handpiece (Figures 6 and 7). Imagine how difficult, or even impossible, it would be to use a straight-nosed handpiece with your endodontic file; that is exactly the problem when a hand file is held improperly.
Pre-curved Hand Files
Gaining access with stainless steel hand files into tight spaces is easier if you curve the hand file than if you attempt to use a straight file (Figures 8 and 9). A curved file is shorter from file handle to file tip, and a curve also makes it easier to “wrap” over mesial marginal ridges as one attempts to enter the endodontic access.
Another option is to use a pen-like handle for a standard hand file. The EndoHandle (Venta Endo) provides an easier grip of a file that can also be pre-curved or bent to facilitate access (Figure 10). With no fingers in the way, the EndoHandle also improves operator visibility into the endodontic access.
Mechanized NiTi Files With Controlled Memory
NiTi mechanized files with controlled memory have been available for several years. These are files that could be curved, and instead of bouncing back to their original straight position, these files remain curved. Hence, the same way that it was recommended to pre-curve stainless steel hand files to more easily gain access into tight spaces, it is strongly recommended that mechanized NiTi files with controlled memory be used. Examples of such files include EndoSequence Reciprocating (ESR) Files (Brasseler USA) and WaveOne Gold (Dentsply Sirona Endodontics). Figure 11 demonstrates how a pre-curved NiTi file can access a posterior tooth more easily.
 |
 |
| Figure 4. Visibility inside an endo access was made possible with enhanced magnification (EXTARO 300 [ZEISS]). | Figure 5. Obturation was facilitated with a small hand mirror and a small carrier-based obturator (GuttaCore [Dentsply Sirona Endodontics]). |
 |
 |
| Figure 6. A stainless steel hand file held at 90° (red lines) to the fingers. | Figure 7. A NiTi file held by a handpiece at 90° (red lines). |
 |
 |
| Figure 8. A pre-curved stainless steel hand file. | Figure 9. View of endo access facilitated with a small mirror as the file is held at 90°. |
Short NiTi Files With Short Shafts
When patients cannot open their mouths very much, every millimeter saved for operating space counts. NiTi files with a shaft that is a few millimeters shorter than conventional-length shafts can make the difference between one being able to perform the endodontic procedure or not. It is recommended that NiTi files with very short shafts be used in cases with limited openings. Furthermore, one should not use a file that is unnec
essarily long. For instance, for a tooth that is 20 mm, one should use a 21-mm file, not a 25-mm file (Figures 12 and 13).
Handpiece With a Small Head
Another way to save a few millimeters when working in a mouth with a limited opening is to use handpieces with small heads. A standard-sized handpiece head could easily be 2 to 4 mm larger than some current-generation motors. For instance, the handpiece head of the recently introduced X-Smart IQ cordless motor (Dentsply Sirona Endodontics) (Figure 14) is significantly smaller than the head of traditional endodontic handpieces.
Enhanced Magnification and Illumination
Pardon the obvious, but visibility in tight and posterior spaces is easily compromised. As such, it is recommended that enhanced magnification and illumination be used. This could be in the form of dental loupes with overhead illumination and/or an operating dental microscope (Figures 3 and 4).
 |
 |
| Figure 10. EndoHandle (Venta Endo) with a bent stainless steel hand file. | Figure 11. This curved NiTi file (WaveOne Gold Glider [Dentsply Sirona Endodontics]) with controlled memory can access a posterior tooth more easily than one that remains straight. Note the improved visibility into endo access with the size 3 mirror. |
 |
 |
| Figure 12. Note differences in shaft lengths of various NiTi mechanized files. Top to bottom: TruNatomy (Dentsply Sirona Endodontics), WaveOne Gold, and XP-3D (Brasseler USA). | Figure 13. While both files are 21 mm, the top file with a longer shaft (blue arrow) is notably longer overall. |
Electronic Apex Locator
Taking radiographs in patients who can’t open their mouths easily could be a challenge. It would also unnecessarily lengthen the procedural time. While pre-, mid-, and post-treatment radiographs are required, it would be helpful if the number of mid-treatment confirmation films could be reduced. This is best achieved with the use of an electronic apex locator.
 |
| Figure 14. Note the small size of the X-Smart IQ endodontic motor head (Dentsply Sirona Endodontics). |
 |
 |
| Figure 15. An 81-year-old gentleman presented for root canal treatment (tooth No. 14) with limited mouth-opening abilities. | Figure 16. Rubber dam isolation was placed. |
CASE REPORT
An 81-year-old gentleman presented for root canal treatment (tooth No. 14) with limited mouth opening abilities (Figure 15). The patient was not able to keep his mouth open for long periods of time. In turn, not only was it important to gain access into the limited space around the tooth, but it was also important to perform the root canal treatment efficiently.
To facilitate access for instrumentation: After the placement of proper isolation for the endodontic treatment (Figure 16), a short (21-mm) stainless steel hand file was used. Initial small size hand instrumentation was achieved with the use of an EndoHandle file holder. A NiTi mechanized file with controlled memory and a short shaft (WaveOne Gold) was used inside an electronic endodontic handpiece (X-Smart iQ) with a very small head.
To facilitate visibility: A small size 3 hand mirror was used to enable visibility into the endo access. Once the file was in the canal, the mirror was moved away to provide more room for hand filing. Also, a dental operating microscope (EXTARO 300 [ZEISS]) was used to enable visibility into the endodontic access and to look for calcified canals. Alternatively, dental loupes with an overhead LED light could also provide enhanced visibility into the endodontic access.
To reduce treatment time and the possible need for numerous mid-treatment radiographs: A NiTi-mechanized filing system requiring fewer files than traditional filing systems was used. In this case, the WaveOne Gold system was used. Note that ESR Files are also designed to require fewer files per routine case. To assist with working length confirmation, an electronic apex locator was used (ProMark [Dentsply Sirona Endodontics]).
To facilitate access for obturation: Carrier-based warm obturation (GuttaCore [Dentsply Sirona Endodontics]) was used. The head of the obturator was removed after the obturator was taken out of the oven. The obturator was handled with cotton pliers. In turn, the obturator was extremely small and very easily maneuvered into the canals. Practically speaking, this obturator was the same size as and handled similarly to placing a paper point into a canal (Figure 5).
When combined, the above tips, tricks, and tools made it possible to predictably, and quite easily, treat the patient with limited access to the posterior tooth.
IN SUMMARY
Gaining access into tight spaces because of limited mouth openings or small mouths is an important challenge to overcome in endodontics. Fortunately, there are many clinical tricks and tools available that help in managing this challenge. Pre-curving stainless steel and NiTi files and using a handpiece with a small head, along with a small hand mirror, can only make it easier for a dentist to perform root canals in such scenarios.
Suggested Reading
- AlRahabi MK. Root canal treatment in elderly patients: a review and clinical considerations. Saudi Med J. 2019;40:217-223.
- Hamedy R, Shakiba B, Pak JG, et al. Prevalence of root canal treatment and periapical radiolucency in elders: a systematic review. Gerodontology. 2016;33:116-127.
- Newton CW, Coil JM. Effects of age and systemic health on endodontics. In: Hargreaves KM, Berman LH, eds. Cohen’s Pathways of the Pulp. 11th ed. St. Louis, MO: Elsevier; 2016:e62-e95.
- Johnson WT, Williamson AE. Isolation, endodontic access, and length determination. In: Torebinejad M, Walton RE, Fouad AF, eds. Endodontics: Principles and Practice. 5th ed. St. Louis, MO: Elsevier Saunders; 2015:244-272.
- Walton RE. Geriatric endodontics. In: Torebinejad M, Walton RE, Fouad AF, eds. Endodontics: Principles and Practice. 5th ed. St. Louis, MO: Elsevier Saunders; 2015:441-454.
Dr. Haas is a certified specialist in endodontics and lectures internationally. He is a Fellow of the Royal College of Dentists of
Canada and is on staff at the University of Toronto Faculty of Dentistry and the Hospital for Sick Children. He maintains a full-time private practice limited to endodontics and microsurgery in Toronto. He can be reached via the website haasendoeducation.com.
Disclosure: Dr. Haas reports no disclosures.
Related Articles
Better and Faster Root Canal Treatments: A Synopsis of the Latest High-Tech Protocols
Clinical Tips for Instrumenting Calcified Canals
The Infamous MB2 Canal: How to Find It and Treat It


