


We are fast approaching the five-year anniversary date of the now famous report by Dr. Mike Barr, “The Inevitable Death of the American Dental Association,” published on The Dental Warrior. This wakeup call was widely discussed by doctors on The Dental Warrior, and also DentalTown.
Dr. Mike Barr
Mike Barr, DDS, formerly very active in Florida organized dentistry, publicly discontinued his membership in the ADA for a variety of reasons. He felt the ADA was too closely aligned with interests outside of general dentists, including the insurance industry, corporate dentistry, and dental specialists.
He also observed that the ADA was advocating for causes outside that of its membership, including the corporatization of dentistry, socialist style healthcare, lesser-trained providers such as dental therapists, and participation in the broken dental Medicaid program, while displaying an unwillingness to promote the benefits of modern dentistry directly to the public.
Barr offered an open challenge to the ADA: “The ADA has a CHOICE. They can either remain on their current course and cling to all the false reasons members are jumping ship. Or, they can STOP, get a little introspective, and TALK to those of us who have left. Your move, ADA.”
On a 2016 Dental Warrior report, Barr followed in his open communication to the ADA with: “My blog written for an audience of dentists averages 10,000 views per month. I am a dental cheerleader. But, I cannot cheer for the ADA. The ADA was lost a long time ago, and deeper in the weeds now than ever before. You’re in deep trouble with MY generation of dentists, and even worse for the younger generation. If you don’t get your (expletive) together SOON, your organization is DEAD. Gone. Soon.”
Barr specifically cited areas of concern for today’s dentists, which the ADA was failing to adequately address:
“1. The INSANELY high cost of dental school, leading to insurmountable debt by new dentists, most of whom will never be able to own their own practices. This has far-reaching effects, including a deleterious influence on the ethics of dentists.
- The growth of ‘corporate dentistry,’ with non-dentists at the helm.
- The increasing interference of insurance companies in the doctor-patient relationship.
- Perpetually increasing regulations by local, state, and national gov’t.
- Our ‘reputation’ or ‘standing’ among professions.
- Increasing vilification of dentists as ‘greedy’ along with increasing attitude that they are entitled to our services.
- The trend towards a ‘single payer’ health system… that some like to include dentistry (a really bad idea).”
Dr. Cynthia Pauley
Cynthia Pauley, DDS, currently serves as president of the Washington State Dental Association. In steep contrast some other elements in organization dentistry, her state’s association has directly engaged in state legislation to protect and preserve the doctor/patient relationship from the interferences of corporate healthcare.
Pauley also has led efforts to confront the dental educational-industrial complex allegedly unfairly operating at the University of Washington School of Dentistry. Her group openly challenged allegedly corrupt practices of Delta Dental through the legal process, regulatory process, legislative process, and direct dissemination of information to the public.
“I believe the ADA is at its best when it is focused on clinical, science-based work or when playing a complementary, supportive role with state and local dental societies. The ADA’s State Public Affairs program, management of a common organized dentistry database, and ADA Seal program are examples of what ADA does well,” Pauley said.
“The governance of the ADA feels increasingly antiquated. The organization has paid for report after report to help it improve its governance and repeatedly fails to implement any meaningful change,” Pauley continued.
“The ADA House of Delegates is too large. The organization has too many committees with too many members. There is also too much duplication between the services provided by the ADA, state dental associations, and local dental societies. Most dues paying members do not understand how all of their ADA dues dollars are spent, and several of the ‘benefits’ provided by the ADA cost extra,” she said.
“In a perfect world, the ADA would find a way to shed some of its legacy costs and divest from duplicative activities performed by state and local organizations. The ADA could then divert those dollars to the highest priorities facing the profession. Reforms require bold action, and so far the ADA House of Delegates has been more interested in preserving the status quo,” Pauley said.
Dr. Gordon Christensen
Gordon Christensen, DDS, MSD, PhD, has dedicated his career to the advance of the dental profession, education of colleagues, and improvements in dental health for the public. In 2011, he presented to the ADA Board of Trustees surveys of thousands of dentists and their frustrations for change within the ADA. Little has changed.
“It is now 2018, and little has changed.” Christiansen added, “WE NEED ACTION AND CHANGE IMMEDIATELY! [emphasis by Christensen].” He then offered the following:
What does the ADA do well?
- Represents the profession and the membership well to the public, politicians, and other health professions
- Provides information about many topics to interested members
- Provides insurance and other benefits
- Attempts to keep members up-to-date relative to political and scientific changes
- Attempts to keep interested members involved in local leadership roles
- Provides continuing education
What aspects need improvement?
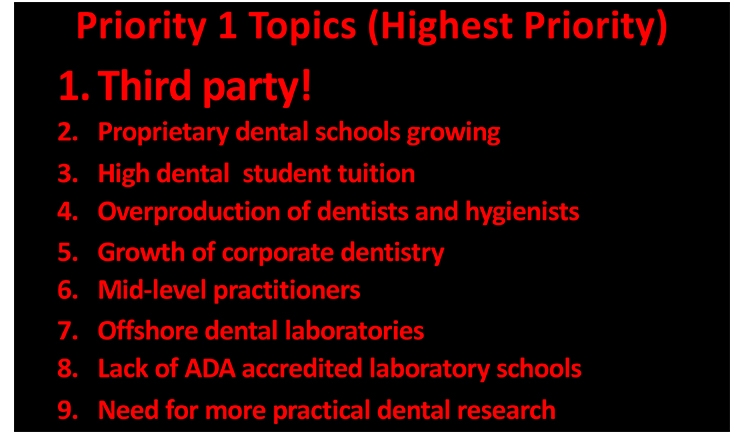
- You could take the red list (priority 1 above), and it well represents the feelings of the profession. As I said, little or nothing has been done on those challenges in the 7+ years since my original survey.
- By far, third-party involvement and domination is the major challenge facing dentistry, limiting quality care because of low fees, keeping dentist net income at the 1997 level (according to the ADA stats), and frustrating treatment plans.
- The oversaturation of dentists is a significant negative factor in many areas of the country.
- High tuition costs are formidable. Funding is necessary.
- More pragmatic clinical teaching and learning in dental schools. The current domination of research in many dental schools has made teaching a minor part of what many faculty members do. Some of the new private schools are turning out better practitioners than the major universities.
- The liberal “do-gooders” and their influence on mid-level practitioners is a misguided concept.
- The profession needs its parent organization, the ADA, to better represent what it actually does rather than “pie-in-the-sky” research and speculation. Note the current ADA journal and try to find something that relates to what dentists actually do. My opinion, after doing dental research for 50 years, is that research should support practice, not the reverse. Now, many federal grants, highly sought after by dental school faculties, support projects that have minor or no relation to practice.
- A major emphasis to get the profession back to a profession with improved ethics and professionalism with less emphasis on $$$.
Will the ADA go the way of the AMA?
- There are currently groups that think so.
- There is currently a movement to rebel against the ADA demanding attention to and action on the points I have previously mentioned.
- In the event the status quo continues, the ADA will continue to lose members.
- Immediate action on the major challenges in the profession is MANDATORY!
Dr. John S. Findley
John S. Findley, DDS, practices general dentistry in Plano, Texas. He is a past president of the Texas Dental Association and the ADA.
“First and foremost, the ADA is uniquely positioned to answer the challenges and effect the changes necessary to keep this profession and the Association a viable and effective force in healthcare in the United States. At this time, no other professional organization in any healthcare field exists with the capacity to accomplish a mission of such significance for an entire profession,” Findley said.
“Similar organizations may exist, but effective representation and thus desired results have been stymied by the loss of member interest and the resulting loss of market share. The ADA has position and standing. It has a critical responsibility and is in a unique position to shape the future,” said Findley.
“The ADA must first continue to represent the interests and fulfill the needs of its members. If that fact is ignored, you will see membership decline and meeting attendance decline. As noble as its many causes are, the ADA is first a members’ organization. Members need to feel, they need to believe, and they need to see that their needs are being answered by their organization,” Findley said.
Findley laid out important specifics.
“Both the busyness and business of our profession are challenging issues for the ADA. I can read the stats and see the numbers, but I also practice and I hear the comments of those in practice. The ADA must gain and keep the leading edge for representing what members believe is important for their practices and the profession,” he said.
“The roles that manufacturers and supply houses play in the dental care arena are now being examined in the court system, and rightly so. The cost of the provision of care is a subject demanding Association attention from the member viewpoint. Education’s role in the profession extends far beyond the classroom. The economic role that education plays in the after-graduation life of a professional should be openly studied and understood,” he said.
“In Congress, notably at the ADA’s continuing instance, we must see the unfair anti-trust exemption extended to the insurance industry be given a fair hearing and hopefully a final resting place. It’s been a long time coming, but the ADA has long-championed repeal of McCarran-Ferguson. Only the ADA is capable of exerting the necessary force to see this happen,” he said.
When asked what the ADA does well, Findley offered, “The ADA continues to be very successful in advocating for the extension of dental care to all—a vital part of our professional foundation. The promotion of the benefit of community water fluoridation has always been given priority in Chicago. An advocacy for quality of care was paramount in the eyes of the founding fathers of our Association. This need continues today. The best example of quality advocacy is what we see in the ADA Seal program. It works. It is a brilliant example of what an Association can do for the profession and the patient.”
He concluded with how he sees the ADA’s future: “(We must) recognize the tenets upon which the Association was founded, be relevant to the daily practice life of members, and promote the well-being of those for whom we care and the demands of the future are met. The ADA can do that!”
Dr. Joseph P. Crowley
Joe Crowley, DDS, has served in organized dentistry for decades and practices in Cincinnati, Ohio. He is the current president of the ADA.
“The future of the American Dental Association is steeped in celebrating diversity and harnessing technology, programs, and partnerships that empower dentists to provide optimal oral health for all,” he said.
“As the demographics of dentistry change, the ADA is focused on demonstrating relevance to women, diverse groups, and new dentists entering the profession. Efforts like the Institute for Diversity in Leadership program, the Women in Dentistry Leadership Series at our annual meeting, and the ADA 10 Under 10 Awards for new dentists are some of the many ways we’re showing up differently to those who may have once thought they couldn’t see themselves in the ADA. The leadership of ADA Councils and Committees is also diversifying, with a 10% increase in the representation of women and a 7% increase in multicultural representation from 2017-2018,” Crowley said.
“We’re also looking to smart technology, innovative policy, and trusted partners to continue proudly serving the profession and the public. From the Find-a-Dentist and ADA Credentialing tools to the Third Party Payer Concierge and insurance provider contract analysis, these services, among others, help to streamline the business side of dentistry,” he said.
“Speaking of the business of dentistry, the ADA is in the midst of launching a pilot program based on field research that found we can play a role in addressing the needs of dentists in making connections. The program will help new and established dentists during their most important transitions, such as finding associates or buying/selling a practice,” he said.
“We’ve also taken concrete actions to advance the overall health of the public, like fighting oral cancer and the opioids crisis and teaming up with partners like CVS Health. Our future is rooted in not only evolving to meet the needs of our changing membership, but taking bold strides to ensure dentists have what they need to do what they do —improve the health of their patients and the overall health of this country,” Crowley said.
Conclusion
Aspects of the dental profession are fully in crisis mode. Immediate and fundamental changes are required. We can’t afford well-intended platitudes of political correctness. A simple quick-fix of a tweak here and there isn’t adequate. The ADA is the single organization best positioned to handle these critical issues, and the time for action is now.
Major tests facing the ADA are on full display. Rank-and-file member doctors demand direct confrontation of these serious matters. If organized dentistry continues to fail membership, membership enrolment will continually bleed away.
The ADA must be very clear on whom it represents without conflicts. Whose interests come first: member doctors (inclusive of the doctor/patient relationship, which involves the public), government programs, the insurance industry, corporate healthcare, corporate sponsors of dental manufacturers and suppliers, or the dental education-industrial complex? A tacit policy of “Jack of all trades, and master of none” is a recipe for irrelevance.
Maintaining and expanding the ADA’s membership isn’t about social “happy hours” or “pep rallies.” Membership depends upon the ADA’s bureaucracy, from the executive director position down, getting involved in direct confrontational problem-solving in the interests of doctors (and the doctor/patient relationship).
When the ADA acts on behalf of interests outside of its membership, doctors are justifiably frustrated. When the ADA offers little to no support for state organizations directly supportive of doctor/patient interests, membership gets very frustrated. That frustration could well portend the demise of the ADA.
Disclosure
The author is a “Life Member” of the ADA.
Dr. Davis practices general dentistry in Santa Fe, NM. He assists as an expert witness in dental fraud and malpractice legal cases. He currently chairs the Santa Fe District Dental Society Peer-Review Committee and serves as a state dental association member to its house of delegates. He extensively writes and lectures on related matters. He may be reached at mwdavisdds@comcast.net or smilesofsantafe.com.
Related Articles
The ADA’s Morning Huddle Focuses on Public Dental Benefits
Dental Grad Achieves $1 Million in Student Loan Debt
Misrepresentations to Consumers: A Dark Side to Dentistry








