



Anyone who is interested in modern endodontics has been exposed to articles touting the technological advances that have been incorporated into the specialty, including CBCT, nickel-titanium rotary instrumentation, various forms of thermoplastic obturation, and digital x-rays. But I find it impossible to lump these “advances” together as a form of collective good.
There is no question that CBCT enables us to evaluate a tooth and the surrounding bone in far more detail than conventional two-dimensional x-rays. Digital x-rays have significantly reduced radiation exposure, providing almost instantaneous images without the need for developer and fixer solutions. At the same time, they can be transmitted via the internet to anyone who may require them. These “advances” are truly beneficial without any downsides.
The Effects of Instrumentation
On the other hand, the incorporation of greater tapered nickel-titanium instruments used in both continuous and interrupted rotation is not, in my opinion, an unquestionable “advance.” Consider some of the effects of such instrumentation:
- Increased incidence of instrument separation
- The removal of significant amounts of dentin beyond what is required to cleanse the canal
- A need to stay centered that compromises the ability to remove pulp tissue in the buccal and lingual extensions
- The incorporation of techniques such as straight-line access and crown-down preparations that, while reducing instrument separations, further weaken the tooth
- The impaction of dentin debris generated from greater tapered mesio-distal preparations into the thin buccal and lingual extensions that compromise the beneficial effects of irrigation.1-12
This is a formidable list that detracts from what advocates call a paradigm improvement over older technology.
Perhaps the least understood impact of greater tapered rotary NiTi instrumentation is its effects on the remaining dentin. Greater tapered rotary instrumentation produces dentinal micro-cracks that can coalesce and propagate into vertical fractures, resulting in the loss of the tooth. This should come as no surprise.
 |
 |
|
Figure 2. The patient was 14 years old with wide canals, but still not exceeding an 02 taper. Bucco-lingually, large isthmuses connected portions of the distal canals. |
 |
|
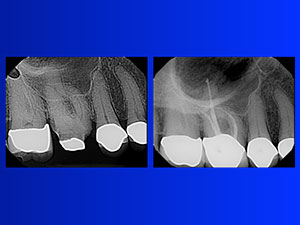
Figure 3. In the third case, we had a dilacerated MB root in the maxillary right first molar. |
Instrument separation via excessive torsional stress and/or cyclic fatigue from an instrument rotating within a canal is well documented. While we understand that the canal walls can negatively impact the integrity of the instrument, what is far less understood is the impact of the instruments on the canal wall.
Newton’s Third Law of Motion tells us that interactive bodies have an equal and opposite impact on each other. It also means that the walls of the canal are as vulnerable to cracks and fractures as the instruments are.
We don’t appreciate this fact because a fractured instrument is immediately obvious, while dentinal cracks are unobservable and often take time before they are seen clinically. To further emphasize this reality, dentin has fatigue properties similar to metal. It is just present in greater bulk.
I don’t believe that any technology described as an advance should carry so much baggage. Of course, a counterargument can be made. Greater tapered rotary instrumentation can often speed up the formerly manual instrumentation process. We should examine that point.
If we are going to compare a manual technique to an engine-driven one, it is highly likely that the engine-driven one will save time and reduce hand fatigue. However, a comparison between greater tapered rotary instrumentation need not be limited to the manual use of files.
The Use of Reamers
In our endodontic office, we employ reamers rather than files. The difference between the two is significant. Reamers have about half the number of flutes along the same 16 mm of working length as a file, with the flutes being twice as vertically oriented.
When used manually, the fewer number of flutes engaging the canal walls results in far less resistance as the instrument negotiates to the apex. These instruments are not limited to manual use. They can be inserted into a 30° handpiece oscillating at 3000 to 4000 cycles per minute.
A frequency as high as 3000 to 4000 cycles per minute provides efficient and effective instrumentation. At the same time, the short arc of motion generated by a 30° oscillating handpiece virtually eliminates the torsional stress and cyclic fatigue that develops in full rotations whether generated in a continuous or interrupted fashion.
Short arcs of horizontal motion virtually eliminate instrument separation. Understanding this fact has several benefits. For example, we eliminate the need for crown-down preparations, which is is another way of saying we preserve significantly more tooth structure.
Crown-down preparations require greater tapered preparations. By substituting 30° oscillation for both continuous and interrupted rotations, we no longer need instruments of greater taper. A 02 taper is more than sufficient to clean any conceivable canal we may be called upon to treat.
By using instruments limited to an 02 taper, we no longer need nickel-titanium. Rather than carving out large amounts of dentin, the thinner 02 tapered stainless-steel reamers act more like internal routers faithfully following the preexisting anatomy in three dimensions and uniformly enlarging the canal so the final preparation is more or less a slightly wider version of the original anatomy.
We preserve tooth structure, remove more pulp tissue particularly bucco-lingually, virtually eliminate instrument separation, do not impact debris bucco-lingually, use the instruments several times before replacement, eliminate hand fatigue from beginning to end, and have significant savings.
One final thought on this alternative approach compared to the use of greater tapered rotary preparations: We place a flat along the entire working length of the reamer. This further reduces the engagement of the instrument along the length of the canal wall, reducing the resistance when negotiating apically.
Also, it creates two vertical blades that shave dentin away in both the clockwise and counterclockwise arcs generated by the 30° oscillating handpiece, improving the efficiency of these reamers. The flat reduces the cross-sectional diameter, increasing the instrument’s already appreciable flexibility and allowing it to negotiate highly curved canals with greater ease.
It takes a detailed explanation to get across the idea that not all technological advances are advances. By adopting the use of relieved stainless steel 02 tapered twisted reamers in a handpiece oscillating at 3000 to 4000 cycles per minute, we have improved the effectiveness of instrumentation while creating conditions that are safer for the tooth and the instrument.
Any system that compromises the strength of the tooth for the increased safety of the instrument is flawed. In our office, we have chosen the alternative pathway discussed above, and we have not looked back.
Thermoplastic Obturation
In a sense, thermoplastic obturation depends on greater tapered preparations producing conical spaces. Given this requirement, the following consequences never made sense to me:
- Thermoplastic obturation results in shrinkage upon cooling that produces gaps that lead to leakage.
- Gutta percha is itself a very poor sealant.
- All thermoplastic techniques are both more complicated and more expensive than non-thermoplastic techniques.
The only justification for increased complexity is a superior and/or more timely result. Neither has been shown to be true. A room temperature single gutta percha point fitting well mesiodistally leaves voids that will be obturated when the canal is flooded with a highly flowable cement prior to the cementation of that single point.
Traditionally, the rationale for the maximum presence of gutta percha was the fact that the cements were susceptible to washout, inducing and exacerbating leakage. By keeping the cement interphase as thin as possible, the gap formed by cement washout would also be minimal.
Today we use polymeric cement resins rather than particulate cements that are highly resistant to cement washout, bond to both dentin and gutta percha, and are dimensionally stable. These facts eliminate the need to adapt gutta percha as closely as possible to the canal walls, reducing the stress the tooth is subject to when employing this form of obturation.
In fact, a single gutta percha point placed in a canal flooded with an epoxy resin cement produces a well-sealed three-dimensional fill that is not prone to shrinkage and, in fact, expands from its room temperature placement as it warms to body temperature. Three cases illustrate a few technique examples.
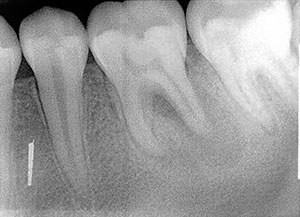
In the first case, the canals in the mandibular right first molar tooth were quite thin mesio-distally (Figure 1). The distal canal had a broad isthmus common to both the disto-buccal and disto-lingual canals. The goal was to remove the tissue in the isthmus common to both canals.
We successfully accomplished this goal because we were able to use the 02 tapered relieved SafeSider reamers aggressively in the bucco-lingual plane from the thinnest initial instrument to the final instrument going sequentially from an 06 tipped 02 tapered SafeSider to a 30 tipped 02 tapered SafeSider. We can do this without concern for instrument separation because the amplitude of motion is limited to 30°.
The second case presented a mandibular left first molar that was the opposite of the first case (Figure 2). The patient was 14 years old with wide canals, but still not exceeding an 02 taper. Bucco-lingually, large isthmuses connected portions of the distal canals.
By preparing the canals from the initial thin 02 tapered SafeSider to a final preparation of a 40 tipped 02 tapered instrument, we were able to thoroughly cleanse the canal in the bucco-lingual plane while preserving tooth structure in the mesio-distal plane.
In the third case, we had a dilacerated MB root in the maxillary right first molar (Figure 3). I included this case to demonstrate the adaptability of the SafeSiders to whatever situation exists. To negotiate this canal, I had to bend the instruments and manually negotiate around the curve. Once around, I was able to attach the instrument directly to the handpiece to more rapidly widen the canal without distortion.
As with all the instruments, they are purposely worked buccally and lingually to remove tissue ensconced in there. Despite the abruptness of the curve, 30° oscillation virtually prevents instrument separation during the shaping process.
Conclusion
A broad spectrum of consequences may result from the application of new endodontic technologies. Once we realize that greater tapered preparations weaken the tooth for the safety of the instrument and that existing alternatives make this approach unnecessary, we can redirect our thinking to a critical appraisal of these other options.
Seeking and finding effective alternatives to greater tapered instrumentation is an exhilarating experience. The same holds true for thermoplastic obturation. By using a room temperature system based on a single master point and a canal thoroughly flooded with an epoxy resin cement, we attain the desired three-dimensional fill in a far more controlled fashion, making the procedure safer and more predictable.
Nothing is gained by prematurely accepting all technological innovations as advances. I have found that the best tool I can use in taking the measure of technological innovations is their compatibility with the most up-to-date goals for effective endodontic therapy. A prime component of those goals is the preservation of tooth structure, both quantitatively and qualitatively.
References
1. Krishna V, Suneelkumar C, Madhusudhana K, et al. Evaluation of dentinal damage after root canal preparation with ProTaper Universal, Twisted files and Mtwo rotary systems—an invitro study. International Journal of Medical and Applied Sciences. 2014;3:146-151.
2, Al-Zaka IM. The effects of canal preparation by different NiTi rotary instruments and reciprocating WaveOne file on the incidence of dentinal defects. Iraqi Academic Scientific Journals. 2012;9:137-142.
3. Çapar İD, Uysal B, Ok E, et al. Effect of the size of the apical enlargement with rotary instruments, single-cone filling, post space preparation with drills, fiber post removal, and root canal filling removal on apical crack initiation and propagation. J Endod. 2015;41:253-256.
4. Ashwinkumar V, Krithikadatta J, Surendran S, et al. Effect of reciprocating file motion on microcrack formation in root canals: an SEM study. Int Endod J. 2014;47:622-627.
5. Barreto MS, Moraes Rdo A, Rosa RA, et al. Vertical root fractures and dentin defects: effects of root canal preparation, filling, and mechanical cycling. J Endod. 2012;38:1135-1139.
6. Liu R, Kaiwar A, Shemesh H, et al. Incidence of apical root cracks and apical dentinal detachments after canal preparation with hand and rotary files at different instrumentation lengths. J Endod. 2013;39:129-132.
7. Bier CA, Shemesh H, Tanomaru-Filho M, et al. The ability of different nickel-titanium rotary instruments to induce dentinal damage during canal preparation. J Endod. 2009;35:236-238.
8. Yoldas O, Yilmaz S, Atakan G, et al. Dentinal microcrack formation during root canal preparations by different NiTi rotary instruments and the self-adjusting file. J Endod. 2012;38:232-235.
9. Shemesh H, Bier CA, Wu MK, et al. The effects of canal preparation and filling on the incidence of dentinal defects. Int Endod J. 2009;42:208-213.
10. Adorno CG, Yoshioka T, Suda H. The effect of root preparation technique and instrumentation length on the development of apical root cracks. J Endod. 2009;35:389-392.
11. Kumaran P, Sivapriya E, Indhramohan J, et al. Dentinal defects before and after rotary root canal instrumentation with three different obturation techniques and two obturating materials. J Conserv Dent. 2013;16:522-526.
12. Bürklein S, Tsotsis P, Schäfer E. Incidence of dentinal defects after root canal preparation: reciprocating versus rotary instrumentation. J Endod. 2013;39:501-504.
Dr. Musikant has lectured worldwide in more than 150 locations and has coauthored more than 300 dental articles published in major dental journals. As a partner in a New York City endodontic practice, his 40-plus years of clinical experience have crafted him into one of the top authorities in endodontics. He’s currently the course director of endodontics at Touro College of Dental Medicine at New York Medical College in Valhalla, NY. He can be reached at (888) 542-6376, via email at the address info@essentialseminars.org, or via the website essentialseminars.org.
Disclosure: Dr. Musikant is president of essential dental systems, which manufactures relieved reamers (SafeSiders) and epoxy resin cement (EZ-Fill).
Related Articles
Endodontic Instrumentation and Obturation Techniques: Do They Conform to Endodontic Principles?
Ten Hints for Endodontic Success
Access: The Good, the Bad, and the Ugly








