

Certainly, there are many options for the restoration of our edentulous patients. Conventional dentures still have a place for some people. Removable implant-retained overdentures are often a positive treatment option improving both form and function and eliminating the prohibitive palate in the maxillary arch. Those patients who request a fixed appliance can benefit from the CAD/CAM technology available to the profession today. Understanding anatomy and implant position—but, most importantly, realizing the emergence profile that is needed to maintain a screw-retained, fixed implant prosthesis will provide for an outstanding final result, a satisfied patient, and a positive long-term prognosis.
Edentulous patients continue to lose bone height and width over time. Facial and lip support are compromised, and vertical dimension of occlusion may decrease. Dental implant reconstruction has become a viable alternative to more conventional techniques and is certainly within the realm of the general practitioner. The essential aspects of implant dentistry today are proper implant position; soft tissue management and health; and knowledgeable dental laboratory technicians who understand the principles of design, form, and function.1
Most of the public today has a fairly sophisticated understanding of the benefits that implant dentistry provides. Marketing and internet searches provide some positive information that directs patients to our practices. In the past, dental implants could be placed to support a removable appliance that had much more stability and function than conventional complete dentures.
However, permanent fixed prostheses are more mainstream than ever before. These appliances have become popular where the anatomy is acceptable and there is enough spacing of the implants to provide for a properly engineered design. Modern technology and materials provide for CAD/CAM design and precise milling of a prosthetic appliance from solid zirconia (BruxZir [Glidewell]).2,3 These full-arch, implant-restored options provide excellent function, easy maintenance, aesthetics, and a long-term resistance to wear. The material is also wear-compatible with the enamel of the opposing dentition.
This bridge is attached to the underlying implants integrated into the bone via custom abutments, which allow the prosthesis to be cemented to place, or with multi-unit abutments, which allow the appliance to be threaded to position.2,4
 |
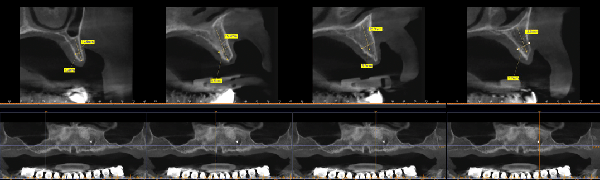 |
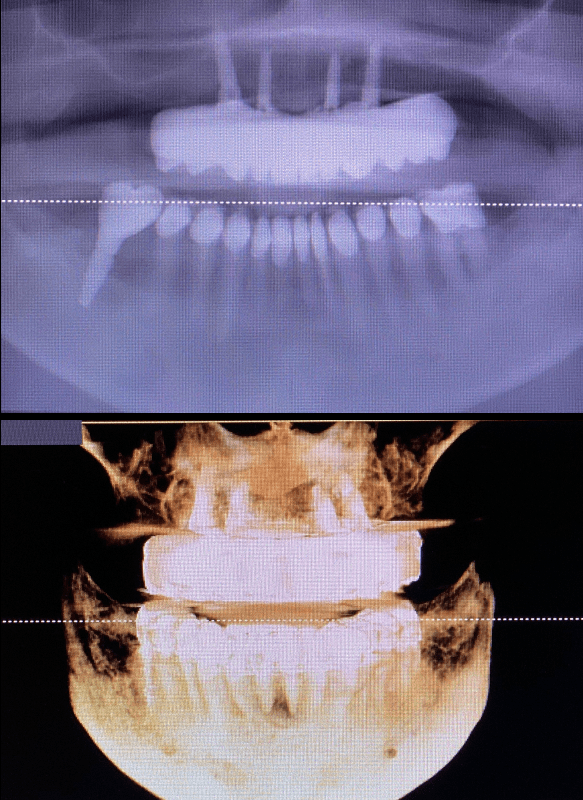
| Figure 1. A preoperative panoramic radiograph indicated potential available bone in the anterior maxilla. | Figure 2. Pre-op CBCT analysis indicated available vertical height of bone but compromised horizontal width. |
 |
 |
| Figure 3. Occlusal view of the edentulous ridge prior to surgical intervention. | Figure 4. The patient’s conventional maxillary complete denture, which she had worn for many years |
Diagnosing and treatment planning are critical to the long-term prognosis of the implant-retained prosthesis. Vital anatomy is reviewed using conventional radiographs, and CBCT analysis allows for visualization of the available bone in the sagittal view. Advances in technology also allow for virtual placement of our implants prior to any surgical intervention. Often, surgical guides can be created to help the practitioner strategically place implants in the best positions.5 Understanding arch form is important to final stability. Misch6 stated that we could predictably cantilever 1.5 times the distance from a line drawn between the 2 most anterior contralateral implants and the most posterior implants in the arch.
Following the strategic surgical placement of dental implants to support a screw-retained, full-arch prosthesis, there are some critical prosthetic applications that the dentist must clearly understand. Depending on the subsequent angulation of the implants in the available hard tissue, the prosthesis can attach directly to the implants themselves or connect to multi-unit abutments when the access holes for the abutment screws are in an unacceptable position. These multi-unit abutments serve to re-angle the abutment screws to a better access on the palatal aspect of the restoration. The connection, strength, long-term periodontal health, and final aesthetics of the prosthesis can be affected by the choice of abutments, so choosing wisely is important.7-9
 |
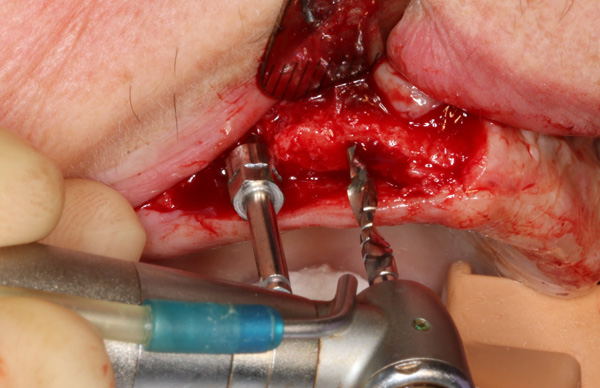 |
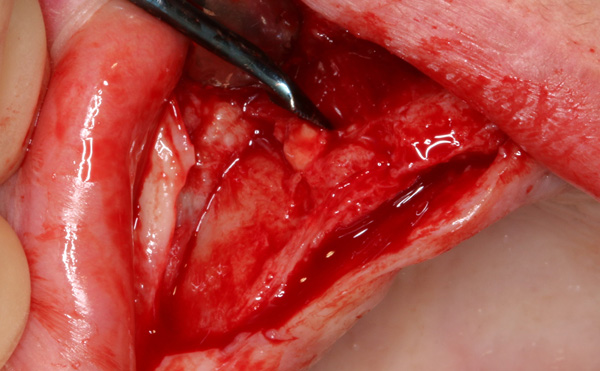
| Figure 5. A reflection was made to visual- ize the available hard tissue. | Figure 6. Without the use of a surgical guide, implants were paralleled using the 2.4-mm-diameter pilot bur from the Hahn Tapered Implant Surgical Kit (Glidewell). |
 |
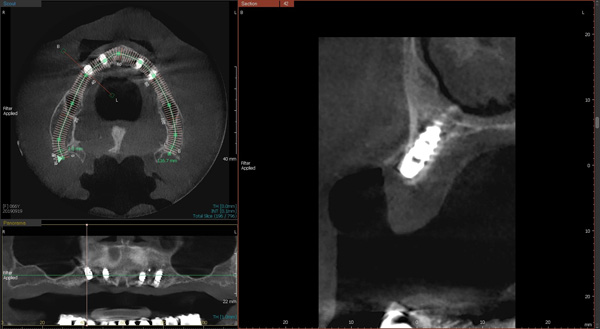 |
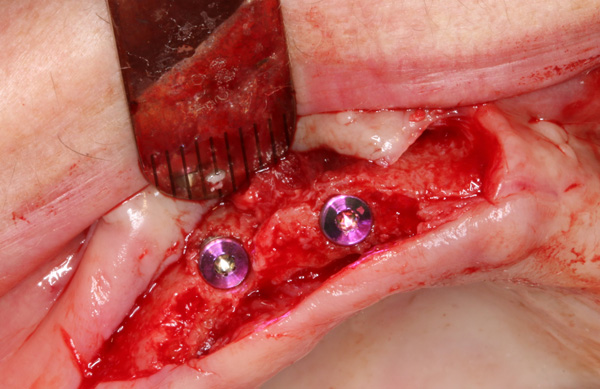
| Figure 7. Following torquing of the implants to approximately 35 Ncm, cover screws were placed into each implant to allow for uninterrupted integration of the newly placed implants. | Figure 8. Postoperative saggital view from the CBCT analysis indicated proper positioning of the 4 strategically placed dental implants. |
BruxZir zirconia provides outstanding strength, wear-resistance, and aesthetics. The appliance is CAD/CAM-designed and milled to the desires of the patient and under the direction of the dentist.10
CASE REPORT
Our patient was a 67-year-old white female with no significant medical or healing findings. Her maxillary conventional denture was barely tolerated for many years. With a better understanding of the benefits that dental implants could provide, she investigated alternatives to improve her quality of life and function without sacrificing the aesthetics she was accustomed to. Implant position was determined prior to any surgical intervention considering the available residual bone and undercuts. It was determined that 4 strategically placed dental implants could support an implant-retained overdenture or a fixed, implant-retained prosthesis.
There are protocols that must be followed to ensure a quality and well-fitting prosthesis that does not stress the underlying implants. The clinical procedures for restoring this maxillary edentulous ridge with a Bruxzir full-arch, implant-retained prosthesis are described in detail. It is essential to follow the steps precisely to ensure an accurate final result.
Our patient presented edentulous in her maxilla for many years. CBCT analysis assessed the patient’s bone volume and position of vital anatomy. The scan allowed me to determine the number of dental implants and the positions in which I would ideally like to place them. Certainly, the information obtained with the CBCT scans could be used to virtually design the implant positions and even the final prosthetic design. However, I decided to surgically place the implants without the use of a prefabricated surgical guide. The literature clearly indicates that the surgical placement of 4 properly spaced implants has an outstanding prognosis for this fixed, implant-retained prosthesis.9,11,12 The patient’s residual ridge exhibited adequate quality and quantity of bone for the placement of implants.
Figures 1 and 2 illustrate the preoperative panoramic radiograph and the sagittal view of the CBCT analysis (Vatech Green CT) (Vatech America). These radiographs indicated the potentially available bone in the anterior maxilla. The occlusal view of the edentulous maxillary ridge prior to any surgical intervention (Figure 3) showed that it would allow for enough interocclusal space to accept a fixed maxillary implant-supported bridge. The patient’s existing denture was evaluated for aesthetics, tooth shape, and position (Figure 4). The patient had no complaints about the aesthetics here. A minimum of 16 mm of interocclusal space is always required per arch for this particular type of fixed prosthesis.
 |
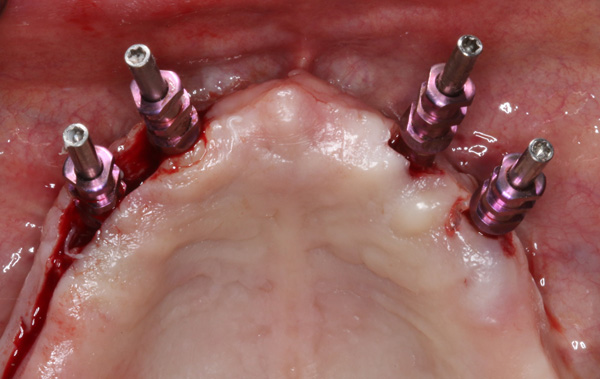 |
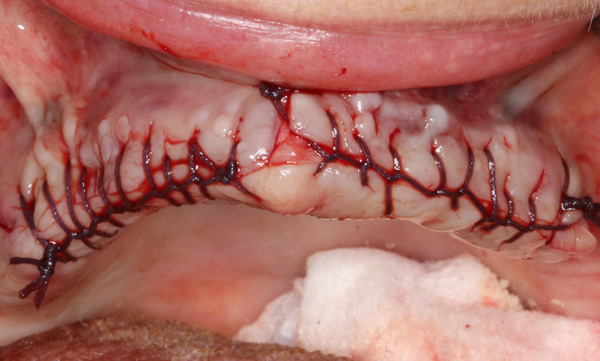
| Figure 9. The tissue reflection was sutured closed using a continuous Vicryl technique. | Figure 10. Following 4 months of inte- gration, the implants were uncovered, and open tray impression copings were engaged into each implant. |
 |
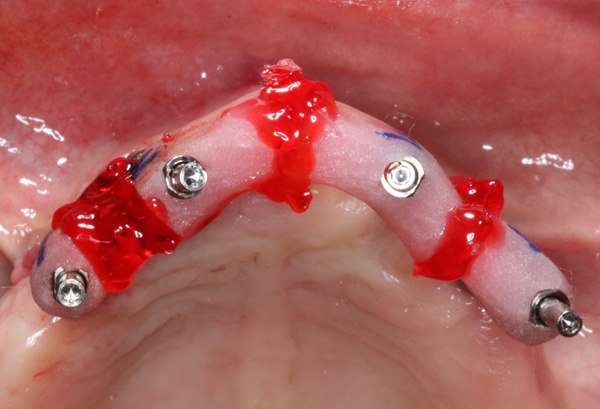 |
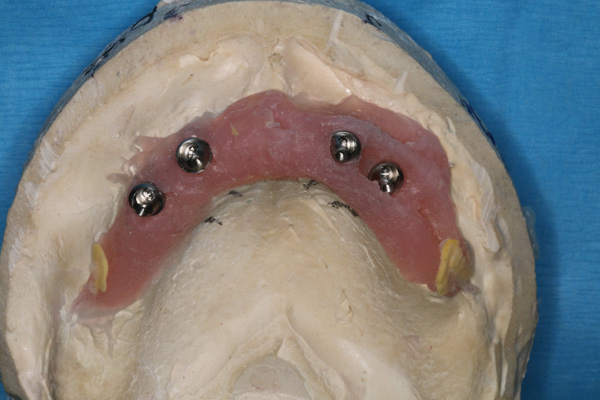
| Figure 11. The dental laboratory (Glidewell) created the preliminary cast and determined the proper multi-unit abut- ments to be used for this screw-retained implant prosthesis. | Figure 12. The laboratory created impres- sion jigs for each implant, which were luted together with flowable composite material chairside to create the final accu- rate master cast that was used to create the final prosthesis. The connection of the final impression coping was checked radiographically. |
With my treatment plan finalized, surgical placement of the implants was started. A reflection was made facially and palatally to expose the available hard tissue (Figure 5). The Hahn Tapered Implant Surgical Kit (Glidewell) was used. A 2.4-mm- diameter pilot bur created the initial osteotomy, allowing for proper mesial-distal and facial-palatal direction. Depth was determined radiographically. Once the first implant was ideally positioned, the subsequent osteotomies were easily completed, paralleling the strategically placed first implant (Figure 6). Since the patient would wear her existing denture during the 4-month integration period, cover screws were threaded into each implant to allow for stress-free healing (Figure 7). Figure 8 demonstrates a postoperative sagittal view of one of the implants in the available bone. A mattress Vicryl suture (Glidewell) was completed, approximating the reflected tissue and maintaining attached gingiva on the facial aspect of the implants (Figure 9). With proper suturing techniques, tissue approximation is excellent after one week. Sutures are removed in 7 to 10 days.
 |
 |
| Figure 13. The laboratory then fabricated a screw-retained occlusal rim that engaged the angled multi-unit abutments, and a conventional denture setup was done to evaluate occlusion and aesthetics. | Figure 14. In a subsequent visit, the screw-retained wax try-in was evaluated. |
 |
 |
| Figure 15. From the wax set-up guide, the lab created a PMMA in composite, which the patient was able to wear for a short time to determine comfort, aesthetics, and function. Any changes to occlusion were easily made chairside. | Figure 16. The transitional appliance was verified with the patient. Access holes were covered with a small cotton pellet and cavit material. This allowed for easy removal and access to the abutment screws for removal. |
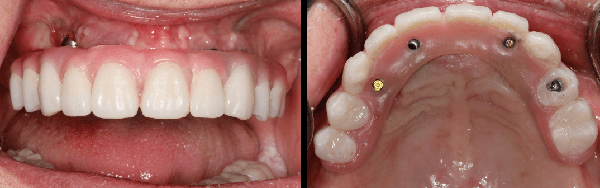
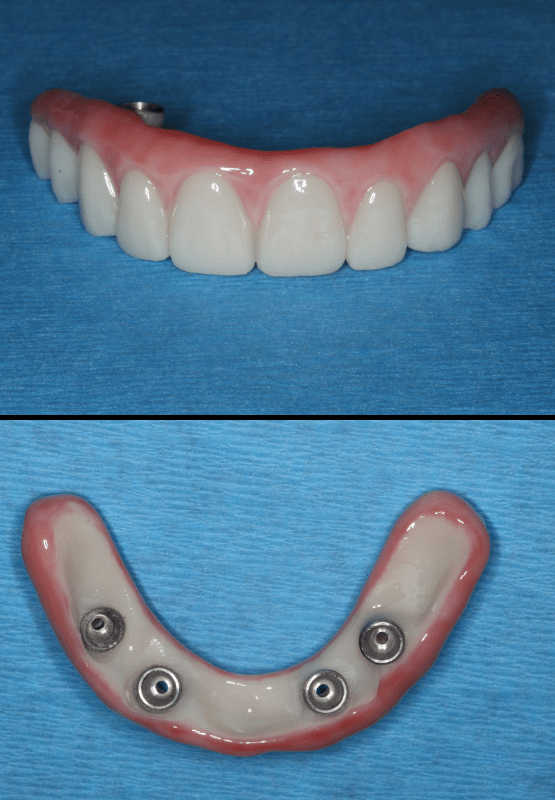
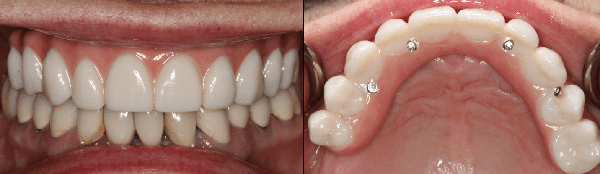
Following 4 months of integration, the implants were uncovered, and open tray impression copings were engaged into each implant (Figure 10). The open tray technique is preferred when multiple implants are placed across the arch and are not in precise parallel position. Glidewell dental lab created the preliminary cast and determined the proper multi-unit abutment height and angulation to be used for this screw-retained implant prosthesis (Figure 11). The lab also created the final impression jigs for each individual implant. These were luted together with a flowable composite material chairside (Primopattern LC Gel [Pri- motec]) to create the final accurate master cast that would be used to create the final, passively fitting prosthesis (Figure 12). The connection of the final impression copings were checked radiographically for a complete seat. The lab then fabricated a screw-retained occlusal rim that engaged the angled multi-unit abutments (Figure 13), and a conventional denture setup was done to evaluate occlusion and aesthetics. Figure 14 illustrates the stable, screw-retained wax setup. From this approved wax setup, the lab then created a poly-methyl methacrylate (PMMA) transitional appliance, which the patient wore for a couple of weeks to evaluate comfort, aesthetics, and function (Figure 15). Any changes to occlusion or design were easily made. The transitional appliance was verified with the patient. Access holes were covered with a small cotton pellet and light-body polyvinylsiloxane impression material (Panasil initial contact regular [Kettenbach LP]). This allowed for easy removal and access to the abutment screws upon removal (Figure 16). Once the patient and the dentist make final approval, the transitional PMMA is returned to the lab for fabrication of the final BruxZir implant-retained prosthesis (Figure 17). Our patient was returned to function and aesthetics with the final screw-retained bridge over the strategically placed implants (Figure 18). Figure 19 shows the final positioning and seat of the prosthesis.
 |
 |
| Figure 17. Once approved by the patient, the transitional PMMA was returned to the lab for fabrication of the final BruxZir implant screw-retained prosthesis. Very little to no adjustments were necessary. | Figure 18. The patient was pleased with the final functional and aesthetic BruxZir implant-retained prosthesis. |
 |
|
| Figure 19. The final CBCT analysis indicated well-positioned and integrated Hahn dental implants supporting this fixed BruxZir zirconia screw-retained prosthesis. |
REFERENCES
1. Tischler M. A maxillary fixed bridge supported by dental implants: treatment sequence and soft tissue considerations. Compend Contin Educ Dent. 2012;33(5):340–4. https://pubmed. ncbi.nlm.nih.gov/22616216/
2. Carames J, Tovar Suinaga L, Yu YC, et al. Clinical advantages and limitations of monolithic zirconia restorations full arch implant supported reconstruction: case series. Int J Dent. 2015;2015:392496. doi:10.1155/2015/392496
3. Wadhwani C. Prosthetic retention options for dental implants. Decisions in Dentistry. 2016;24-26.
4. Egilmez F, Ergun G, Cekic-Nagas I, et al. Implant-supported hybrid prosthesis: con- ventional treatment method for borderline cases. Eur J Dent. 2015;9(3):442-448. doi:10.4103/1305-7456.163324
5. Javed F, Ahmed HB, Crespi R, et al. Role of pri- mary stability for successful osseointegration of dental implants: Factors of influence and evalu- ation. Interv Med Appl Sci. 2013;5(4):162–7. doi:10.1556/IMAS.5.2013.4.3
6. Misch CE. Contemporary Implant Dentistry. 3rd ed. Mosby Elsevier; 2008.
7. Limmer B, Sanders AE, Reside G, et al. Com- plications and patient-centered outcomes with an implant-supported monolithic zirconia fixed dental prosthesis: 1 year results. J Prosthodont. 2014;23(4):267–75. doi:10.1111/jopr.12110
8. Oh SH, Kim Y, Park JY, et al. Comparison of fixed implant-supported prostheses, removable implant-supported prostheses, and complete dentures: patient satisfaction and oral health- related quality of life. Clin Oral Implants Res. 2016;27(2):e31-7. doi:10.1111/clr.12514
9. Preciado A, Del Río J, Lynch CD, et al. Impact of various screwed implant prostheses on oral health-related quality of life as measured with the QoLIP-10 and OHIP-14 scales: a cross-sec- tional study. J Dent. 2013;41(12):1196–207. doi:10.1016/j.jdent.2013.08.026
10.Agustín-Panadero R, Román-Rodríguez JL, Fer- reiroa A, et al. Zirconia in fixed prosthesis. A liter- ature review. J Clin Exp Dent. 2014;6(1):e66-73. doi:10.4317/jced.51304
11. Wilson TG Jr. The positive relationship between excess cement and peri-implant disease: a prospective clinical endoscopic study. J Peri- odontol. 2009;80(9):1388–92. doi:10.1902/ jop.2009.090115
12. Balshi TJ, Wolfinger GJ, Slauch RW, et al. A ret- rospective analysis of 800 Brånemark System implants following the All-on-Four protocol. J Prosthodont. 2014;23(2):83–8. doi:10.1111/
jopr.12089
ABOUT THE AUTHOR
Dr. Tilley is a graduate of the University of Alabama School of Dentistry. She is a native of Pensacola, Fla, and has been practic- ing dentistry in her hometown since 1998. She keeps up with the latest in dentistry by attending continuing education seminars on topics such as oral surgery, implants, veneers, periodontal disease, cosmetic pro- cedures, and much more. Dr. Tilley has also done extensive training at the Las Vegas Institute for Advanced Dental Studies and the Engel Institute with Drs. Timothy Kosinski and Todd Engel. She is a Fellow of the International College of Dentists (ICD) and is member of the AGD, the ADA, the Florida Dental Association, the Alabama Dental Association, the Academy of Laser Dentistry, and the Academy of American Facial Esthetics. Dr. Tilley has received a fellowship with the International College of Oral Implantologists and the ICD and has published extensively on implant dentistry techniques, lasers, and Botox/fillers.
She can be reached via email at [email protected].

