


INTRODUCTION
In the practice of endodontics, having the right instruments and an understanding of how to use them is what often differentiates the novice from the master. It was not until the mid-1990s that the majority of us began to realize that NiTi rotary instrumentation was going to be a true game changer. Even then, it took the better part of the following decade for most of us to transition to instruments made of this exotic metal. This was understandable, given that stainless steel hand files and reamers had dominated the landscape of canal preparation for nearly a century.
When first observed, endodontic instruments made from NiTi seem to hail from an extraterrestrial world. They exhibit very unusual properties: shape memory and superelasticity. The shape memory property allows the instrument to “remember” its original shape and retain it when heated above its transformation temperature (Figure 1). In addition, NiTi instruments demonstrate an incredible elasticity that is many times greater than stainless steel.1-3 When combined with an engine-driven handpiece, NiTi instruments are ideally suited for the task of root canal debridement.
Fast Versus Efficient
In an effort to fully exploit the uniqueness of NiTi, the dental industry created more instrument designs and systems to make things easier, faster, and better. There was only one problem: It did not take long before many practitioners realized that easier and faster did not always translate to better. There is a big difference between doing something faster versus more efficiently. Fast is just that—fast. It does not qualify the result! Something that is accomplished more efficiently, on the other hand, specifically addresses that the task accomplished is at least of equal or better outcome. Many of us have confused fast with efficient. This misunderstanding has led to many practitioners using rotary instruments and/or instrumentation systems that remove excessive and important pericervical (coronal root) dentin in their root canal procedures. The result has been the loss of many teeth that have been structurally compromised as a result of using more aggressive instrumentation systems that create larger and excessively tapered preparations (Figures 2 and 3).
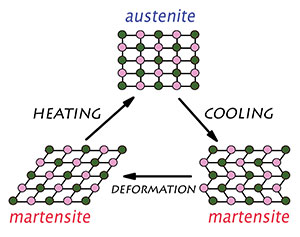 |
| Figure 1. Phase transition of the NiTi alloy from austenite (A) to martensite (M) and back is responsible for this alloy’s superplastic and shape memory characteristics. |
 |
 |
| Figures 2 and 3. (Cases 1 and 2) Excessive coronal taper creates weak areas that can lead to horizontal root fractures (Figure 2) and vertical root fractures (Figure 3). |
Variable Versus Constant Tapered Systems
Over-engagement (leading to excessive torque on a file) can be a potential problem when utilizing some constant tapered file systems. Some manufacturers introduced variable tapered file systems utilizing larger tapers (.12, .10, .08, .06) to overcome this potential problem (Figure 4). It is true that utilizing variable tapers can reduce over-engagement (when used in a crown-down sequence), but they often can lead to the unfortunate consequence of removing excessive cervical root dentin because of their large tapers. For years, the excessive removal of coronal root dentin was considered of little consequence until it was discovered that more and more endodontically treated teeth required extractions resulting from root fractures. No longer did our profession have to address “the pain” of root canals, but the reputation of them not working (Figure 5).
 |
| Figure 4. Variable taper preparations create variable shapes, requiring customized cone fitting for obturation. Constant taper preparations prepare predictable shapes for matching cones and obturation. |
 |
 |
| Figure 5. (Case 3) Radiographs showing a fractured root and over prepared canals. Removal of excessive dentin in the cervical third of the root weakens and predisposes roots to horizontal and vertical root fractures. |
Obturation Dictates Shape
In addition to the above concern, some instrument systems promote the use of “coronal flaring” to facilitate canal preparation and/or the use of the pluggers and spreaders required for various obturation techniques. Larger orifices make it easier to get pluggers and/or spreaders to the apical third of the root canal (for “warm vertical and cold lateral” condensation). Up until now, little concern has been expressed about the excessive removal of pericervical root dentin to accommodate these obturation techniques. Stripping a carrier of its heated gutta-percha is likewise of less concern when the orifice is larger.
 |
 |
| Figure 6. (Case 4) Constant tapered .04 preparation. Narrower, constant taper .04 preparations do not remove important pericervical dentin. |
 |
| Figure 7. The modern nanoparticulate bioceramics have revolutionized the nonsurgical and surgical aspects of obturation and root repair (EndoSequence BC Sealer/Filler and BC Root Repair Material [Brasseler USA]). |
 |
 |
| Figure 8. (Case 5) The integrity of the root can be maintained by using synchronized hydraulic condensation. It does not require larger access for pluggers and spreaders. |
Thus traditional obturation techniques (and their requirements) began to dictate the size and shape of root canal preparations. Idealy, root canal preparations (both size and shape) should be determined solely by the amount of dentin removal required to debride and disinfect the root canal system. How many times were you told that you needed to “shape to obturate”? Instead, what we should have been hearing was that we need to “shape to clean.” Obturation should not dictate shape. In the past, it has been problematic for many (if not most) practitioners to obturate conservative root canal preparations. Advanced material science, in the form of bioceramic technology, has finally unleashed the full potential of NiTi and its ability to produce conservative, less invasive root canal preparations (Figure 6).
Bonded Obturation: Bioceramic Sealers and Fillers
Bioceramics are inorganic ceramic materials specifically designed for use in medicine and dentistry. Examples include zirconia, calcium silicate, calcium phosphate, hydroxyapatite, and bioactive glasses. You may be familiar with mineral trioxide aggregate (MTA); MTA is a rudimentary and early example of a bioceramic compound that has been used in dentistry for apical surgery. Often difficult to manipulate because of its large particle size, early on it represented a significant improvement over amalgam for apical surgery and certain specialty applications. Until recently, its large particle size precluded its use as a sealer. This year it has become available as a sealer, but only as a powder and liquid that requires mixing at the time of use.
 |
 |
 |
| Figure 9. (Case 6) Endo-perio lesion. Compromised supporting structure makes this tooth a perfect candidate for a passive obturation technique (synchronized hydraulic condensation). (a) Diagnostic. (b) Post-op. (c) One-year recall. |
A next-generation nanoparticle bioceramic, EndoSequence BC Sealer/Filler and EndoSequence BC Root Repair Material (BCRRM), is marketed by Brasseler USA. It is available in multiple viscosities for different applications. The distinguishing factor between the various viscosities (hydraulic sealer through root repair putty) is the nanoparticle size of the inorganic ceramic components. What is unique and what distinguishes BC Sealer and BCRRM from all other similar compounds is not only their nanoparticle technology but that they are premixed and ready to be used for all applications (Figure 7). Some of the physical and chemical properties of BC Sealer include that it is: hydrophilic, antimicrobial, stable (does not shrink upon setting), nonresorbable, biocompatible, bonds to dentin, forms hydroxyapatite, and hydraulic due to its nanoparticle size. These attributes (as well as many others) have made this an ideal material to hydraulically seal the root canal space.
Hydraulic Condensation
Hydraulic condensation utilizing BC Sealer/Filler obviates the need for condensation techniques that were previously required to “minimize the sealer interface.” What is so revolutionary is that advanced material science (nanoparticle bioceramic compounds) have made traditional obturation techniques obsolete, given that these materials can act as both a sealer and a filler. BC Sealer/Filler does not exhibit any of the issues that traditional eugenol and resin-based sealers have exhibited, requiring them to be reduced (minimized) in the root canal space; these include shrinking upon setting, lack of biocompatibility, cytotoxicity, hydrophobic nature, lack of antimicrobial activity, and many more well known to most of us. A significant result of this remarkable innovation is that it is now much easier and more efficient to fill conservative “minimally invasive” canal preparations with cold (room temperature) hydraulic condensation (Figures 8 and 9). Of equal importance is the strengthening of the root as the result of the sealer bonding directly to the root dentin and the bioceramic-coated gutta-percha, which forms hydroxyapatite upon setting.4,5
Note: EndoSequence BC Gutta Percha Cones Series 150 (Brasseler USA) are available for warm vertical condensation users/advocates. They are not as stiff as regular BC Gutta Percha, but will melt at a lower temperature (150° rather than 250°C). Since the BC Sealer is hydrophilic, the lower heat requirement for melting the gutta-percha will not desiccate the bioceramic sealer during warm vertical obturation techniques (Figure 10).
 |
| Figure 10. Bioceramic coated gutta-percha cones and pellets are now available at lower melting temperature of 150°C. This combination allows implementation of warm vertical compaction with bioceramic-based sealers. |
 |
| Figure 11. Heat treatment of a NiTi file changes the alloy property at room temperature and therefore the file’s behavior. These changes have some advantages and disadvantages, depending on the specific clinical situation present. |
SHAPE MEMORY VERSUS CONTROLLED MEMORY
Today, NiTi rotary instruments are the most popular material/method for mechanical root canal debridement. In the current market, NiTi instruments are available along a large spectrum that spans a pure austenitic (A) phase rotary file to a pure martensitic (M) phase instrument (Figure 11). These 2 forms represent 2 crystalline structures of the same nickel titanium metal, each with different characteristics. Traditional NiTi files are in the A phase and are referred to as shape memory files. Recently, files have been introduced that are heat-treated to change their crystalline phase to M, and these files are referred to as controlled memory files. The clinical performance (differences) between 2 files of similar design and size can be remarkable depending on their phase state (A or M). In general, A-files are more resistant to torque and less resistant to cyclic fatigue, while M-files are just the opposite. Also, A-files will be stiffer and sharper than M-files of similar size and shape.
So, A and M rotary files are best used in different circumstances: A-files will serve you best when you want to be as efficient as possible (basic to moderately advanced cases), while M-files will rise to their best advantage when treating severely curved canals (more advanced cases). But more to the point, it makes little sense to use an A-phase file in a very curved canal or an M-phase file in a basic (straight) case.
ESX: Shape Memory
The ESX rotary file system (Brasseler USA) was designed for maximal efficiency while producing a very conservative “minimally invasive” (.04 constant taper) shape (Figure 12). The patented “Booster Tip” enhances the A-file’s ability to follow the canal’s natural morphology (Figure 13). The ESX rotary file system utilizes a patented alternate contact point design that reduces engagement by 50% while providing a safe, efficient, and minimally invasive preparation (Figure 14).6-8
For most basic cases, the ESX system will require only 2 files, the Expeditor and one of the finishing files (small, medium, or large) to accomplish the shaping of the root canal. A more advanced calcified case will require the incorporation of the ESX Scout instruments to prepare the canal for the Expeditor. If your case is severely curved, it is time to be thinking about adding a controlled memory M-phase instrument (such as KontrolFlex [Brasseler USA]) to your armamentarium (Figure 15).
 |
 |
| Figure 12. (Case 7) Calcified bicuspid (3 canals). Conservative preparation with ESX rotary file system (Brasseler USA) does not weaken the root. |
 |
| Figure 13. Booster Tip is a patented design feature of the ESX that creates 6 cutting edges at the tip to guide the file and reduce ledging potential while centering the file tip and allowing a more gradual taper to the International Organization for Standardization size than traditional tips. The ESX File is electropolished and the Booster Tip helps center the tip through flattened transitions angles. |
 |
| Figure 14. The patented alternate contact point (ACP) design helps reduce file engagement on a constant taper file and prevents taper lock. Alternating cutting points are reduced, thus creating a constant taper during rotation while reducing torque caused by engagement. |
 |
| Figure 15. Basic advanced and advanced squared protocols: Canals with higher degrees of difficulty require additional files and protocol to achieve safe and efficient instrumentation. |
KontrolFlex: Controlled Memory
KontrolFlex rotary files are heat-treated, so they are in their M phase. They are available in 2 series, designated as series one and series two. The first is a pure version of a heat-treated file that results in a very flexible, cyclic fatigue resistant instrument. It is ideal for extreme curves, getting around ledges, and difficult access (Figure 16). It can be precurved and will hold its curve once placed as well as any file available. As a pure M-phase instrument, it will be very flexible, but softer and subject to unwinding easier than some other M-phase instruments (the new EndoSync motor [Brasseler USA] virtually eliminates any issue of unwinding—see next section). It is even possible to put a “J hook” on the tip similar to a stainless steel hand file. The series two instrument is more efficient (more torque resistant) and less susceptible to unwinding, but not quite as flexible (Figure 17).
 |
 |
 |
| Figure 16. (Case 8) Dilacerated root (instrumentation and obturation). Severely curved canal successfully treated using ESX/KontrolFlex files (Brasseler USA) and EndoSequence BC Sealer/Gutta Percha (Brasseler USA). (a) Pre-op. (b) Working length radiograph. (c) Post-op. |
 |
| Figure 17. KontrolFlex: M-files are much more flexible and have controlled memory at room temperature. This allows pre-bending of the file prior to its use. |
 |
| Figure 18. EndoSync motor and A. I. apex locator (Brasseler USA). |
ROTATION VERSUS RECIPROCATION
Continuous rotation is the ideal motion for root canal debridement because the debris generated is removed coronally with every rotation, but continuous rotation can put more torsional stress on an instrument if it is over-engaged. Continuous reciprocation, on the other hand, can reduce the torsional stress on instruments, but compared to continuous rotation, it has some clear disadvantages. Continuous reciprocation has been identified as producing a higher instance of apical debris extrusion, higher postoperative sensitivity, dentinal microcracks, and canal transportation.9-11
EndoSync is the recently introduced “intelligent” cordless endo handpiece that provides all of the benefits of continuous rotation and reciprocation without any of the associated disadvantages. Instead of providing continuous reciprocation with its associated shortcomings, the motor only reciprocates if it senses the need. The handpiece overcomes the inherent disadvantages of each crystalline phase (A or M) by using optimized torque reverse (OTR) technology.
The EndoSync handpiece provides continuous clockwise rotation until a selected torque limit is met and only then will the file go into a reciprocating motion. Once the excessive stress has been overcome, the motor will return instantaneously to its preferred clockwise rotation. This patented intuitive disengagement technology is called OTR. Essentially, it provides continuous rotation when you want it and reciprocation only when you need it for safety. A second but important feature of the EndoSync motor is that it can communicate directly with the EndoSync A. I. (apex locator) (Brasseler USA) to provide continuous monitoring of the anatomical apex (Figure 18). At the operator’s discretion, the A. I. apex locator can be set to slow down and/or stop the handpiece when the apex is reached.
CLOSING COMMENTS
Smart OTR technology and advanced metallurgy (A and M rotary files) have for the first time allowed motion and metal to work in perfect harmony. The synergy achieved between advanced material science (BC Sealer/Filler) and metallurgy (ESX/KontrolFlex) has now allowed endodontic instrumentation to reach its full potential. Root canal treatment can now be considered a fundamental component of the restoration of the tooth, rather than a separate pre-restoration procedure. As we like to say, the restoration of an endodontically treated tooth should begin at the apex.
Acknowledgment
All clinical cases provided by Bradley Trattner, DDS.
References
- Shen Y, Zhou HM, Zheng YF, et al. Metallurgical characterization of controlled memory wire nickel-titanium rotary instruments. J Endod. 2011;37:1566-1571.
- Santos Lde A, Bahia MG, de Las Casas EB, et al. Comparison of the mechanical behavior between controlled memory and superelastic nickel-titanium files via finite element analysis. J Endod. 2013;39:1444-1447.
- Lopes HP, Lopes WSP, Vieira VTL, et al. Evaluation of the flexibility, cyclic fatigue, and torsional resistance of rotary endodontic files made of different nickel-titanium alloys. Int J Dentistry Oral Sci. 2016;S8:001, 1-5.
- Koch KA, Brave DG, Nasseh AA. Bioceramic technology: closing the endo-restorative circle, part 1. Dent Today. 2010;29:100-105.
- Koch KA, Brave DG, Nasseh AA. Bioceramic technology: closing the endo-restorative circle, part 2. Dent Today. 2010;29:98-105.
- Koch KA, Brave DG. Real World EndoSequence file. Dent Clin North Am. 2004;48:159-182.
- Koch K, Brave D. The EndoSequence file: a guide to clinical use. Compend Contin Educ Dent. 2004;25:811-813.
- Koch K, Brave D. Endodontic synchronicity. Compendium. 2005;26:218-224.
- Robinson JP, Lumley PJ, Cooper PR, et al. Reciprocating root canal technique induces greater debris accumulation than a continuous rotary technique as assessed by 3-dimensional micro-computed tomography. J Endod. 2013;39:1067-1070.
- Berutti E, Chiandussi G, Paolino DS, et al. Effect of canal length and curvature on working length alteration with WaveOne reciprocating files. J Endod. 2011;37:1687-1690.
- Bürklein S, Tsotsis P, Schäfer E. Incidence of dentinal defects after root canal preparation: reciprocating versus rotary instrumentation. J Endod. 2013;39:501-504.
Dr. Brave is a Diplomate of the American Board of Endodontics and is a member of its College of Diplomates. In addition to having served as the managing partner of an endodontic specialty group practice for more than 25 years, he has been a prolific author and international lecturer. He is a co-founder of Real World Endo; holds multiple dental patents, including the VisiFrame; and was the first of his colleagues to be named “Baltimore’s Best Endodontist” by Baltimore Magazine. Formerly having served as an associate clinical professor at the University of Pennsylvania’s School of Dental Medicine and having a clinical appointment at The Johns Hopkins Hospital, he now serves as an advisor to Real World Endo. He can be reached via the website realworldendo.com.
Disclosure: Dr. Brave is a consultant to Brasseler USA.
Dr. Trattner received both his DDS and certificate in endodontics from the University of Maryland School of Dentistry. He has maintained a private practice in endodontics in Baltimore for more than 25 years. A Diplomate of the American Board of Endodontics and a member of the College of Diplomates, he holds staff positions at Sinai Hospital and teaches endodontics at the University of Maryland School of Dentistry. He is a past president of the Maryland Association of Endodontists, the Alpha Omega Dental Fraternity, and the University of Maryland School of Dentistry Alumni Board. He is a member of the Pierre Fauchard International Honor Academy and is a Fellow of the American College of Dentists. He has lectured extensively nationally and is a clinical advisor and certified lecturer for Real World Endo. He can be reached at (410) 653-2020.
Disclosure: Dr. Trattner reports no disclosures.
Also By Dr. Brave
Bioceramics, Part 1: The Clinician’s Viewpoint
Bioceramics Part 2: The Clinician’s Viewpoint
A New Endodontic Obturation Technique








