
Implant placement challenges can arise related to a multitude of factors. Those can include short available height related to anatomical structures, narrow available space between adjacent teeth, low density bone that will hamper stability at placement for finned (non-threaded) pressfit style implants and angulation issues. Quantum implants’ features and design aid in overcoming those clinical challenges, providing options in the implant to fit all clinical situations. In addition, the Morse taper connection and slopping shoulder of the implant in combination with Quantum’s Osteosupportive Thread prevents crestal bone breakdown, while maintaining healthy gingiva.
IMPLANT SURFACE DESIGN AND INITIAL STABILITY
Implant stability at placement allows for immediate loading when accepted insertion torque can be achieved. Implants that are pressed (vs threaded) into osteotomies are not able to achieve sufficient insertion torque to allow for immediate loading, whether the surface is coated, treated to roughen it, or has non-threaded surface features such as fins or beads. Additionally, intimate contact of the bone with the entire surface of the implant during placement, allows quicker maturation of the bone at the implant interface.
When a non-threaded implant is placed, a clot lies between the implant surface and the osteotomy on part of the implant surface closer to the implants core, which will require conversion to host bone, delaying the integration period.
Although, Quantum does offer a pressfit finned style implant, the Quantum threaded version offers advantages such as providing immediate stability to permit perfect immediate loading when an acceptable insertion torque level can be achieved. In lower density bone such as found in the maxillary sinus area, when augmentation is to be supplemented at implant placement, it aids in lateral condensation of the bone and initial stability. The potential complications caused by accidental displacement of the implant into the sinus, as can occur with a pressfit finned implant, are greatly minimized or eliminated with the threaded implant design.
The thread geometry of the Quantum implant has deep threads that are spaced to allow for greater initial stability than thread designs that are shallower and more closely spaced. Thread spacing allows for formation of true Harvesian canals between the threads, so circulatory flow in that bone provides for better stability long-term and is easier to maintain under function. Additionally, the deeper threads increase surface area at the bone-implant interface, which combined with the lower surface of the threads being flat, provide high compressive load management of the implant when loaded. (Figure 1)
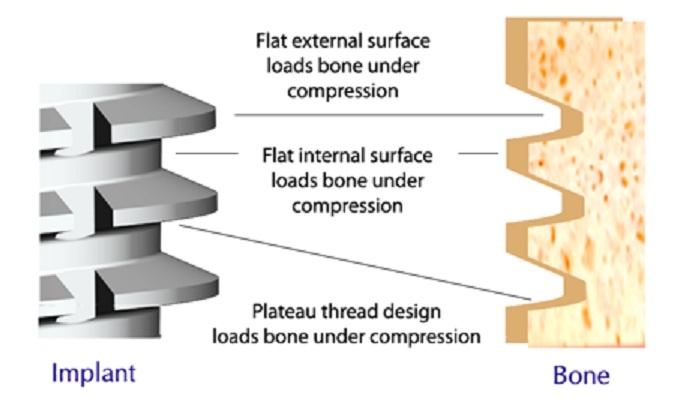
The implant’s design with a flat apex on all the versions improves compressive loading under function. The self-tapping design aids in placement in dense bone with osseocompression in all bone densities for improved bone quality at the bone-implant interface with better initial stability.
The surface treatment of the implant by the manufacturer has been shown to improve clot contact with the implant at placement and subsequently osteoblasts cell adhesion and the quality of the bone-implant interface. Several surface treatments are available with Quantum implants; resorbable blast media (RBM), hydroxyapatite (HA), and biological titanium interface (BioTi). BioTi is a proprietary acid etch implant surface treatment to provide ideal roughness for enhanced bone-implant interface.
This process involves two rounds of acid etching and passivation to maximize the surface for bone adhesion during integration.
3-IN-ONE ABUTMENT CONNECTION
Quantum has a unique implant platform design allowing 3 different abutment connections on the same implant, expanding prosthetic options during planning or following implant placement. This is available on their Summa, Slim, and Short-T implant lines. Their 3-in-One connection offers a choice of using a Morse taper (TaperLock), a taper abutment with threaded terminal end (TaperLock Thread), or an external hex (Hex). (Figure 2)
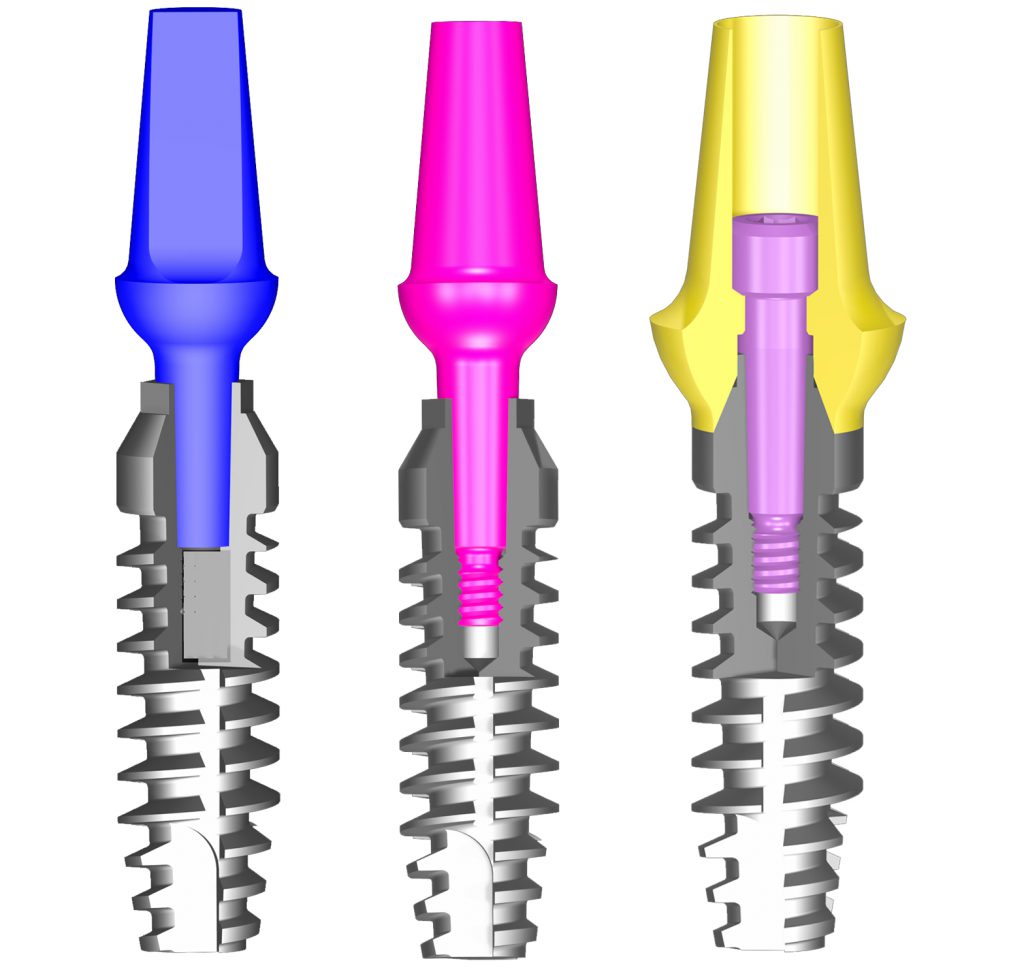
The Hex connector, when utilized, causes the abutment to engage the sloped (bevel) of the coronal aspect of the implant, acting as a reverse internal hex.
The option of the three abutment connections simplifies abutment selection, so depending on available bone, implant angulation, and type of restoration (fixed, removable, hybrid) – the same implant can be restored. This enables the practitioner to modify the treatment plan during the surgery, or the restorative phase, while using the same implant.
The TaperLock connector utilizes a true Morse 1.5-degree taper connection between the abutment and implant at the platform. This allows a solid abutment head without a screw for a rigid connection, while permitting 360° positioning of an angled abutment head to best position the head for either a cemented implant crown, an overdenture, or a QFit regardless of the angulation of the implant to the desired prosthetic vertical axis.
Once the head is positioned at the correct orientation circumferentially, the head is gently tapped into the implant to frictionally engage the Morse taper connector. When this connector option is selected on the implant, the implant is placed subcrestally, so that when the abutment is inserted, the restorative margin on the abutment is positioned subgingivally.
The solid abutments are available in 0° (straight), 15°, and 25° angulations and different lengths. Abutments are preparable to further customize either the length of the restorative portion of the head, or to aid in paralleling adjacent implants that will connected in a bridge.
The frictional fit between the abutment post and implant connector ensures no microgap providing a hermetic bacterial seal at the connector.
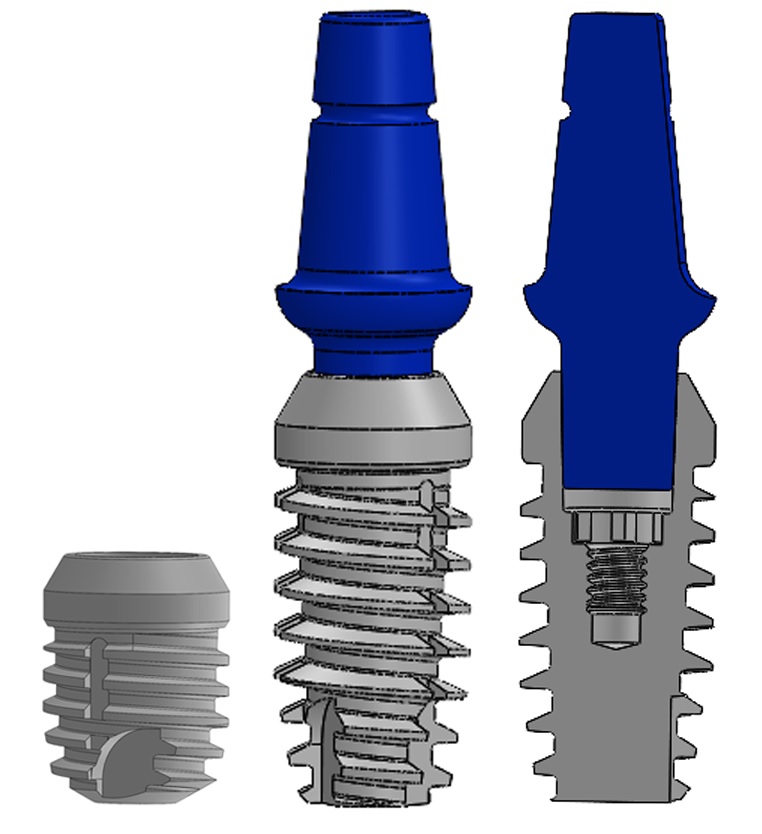
The TaperLock Threaded connector is similar to the TaperLock with a solid abutment head but has a threaded portion at the apical end to allow the practitioner to tighten the abutment to the implant, which provides a rigid connection with extra retention. When this connector option is to be utilized like the TapeLock option, the implant is placed subcrestally. The abutment is provided either as a straight abutment or a custom TaperLock Threaded abutment. This version allows the practitioner to create a custom abutment chairside to accommodate any angulation of the implant in relation to the needed prosthetic axis required. The TaperLock Threaded custom abutment is placed into the implant and tightened prior to any customization. Once secured, the abutment is modified with a carbide bur in a highspeed handpiece, preparing it similarly as a tooth would be prepared for a crown. (Figure 3)
The sloping shoulder combined with the diameter of the TaperLock and TaperLock Threaded post at its mergence from the implant provide true platform switching when these options are selected. This allows greater bone thickness in the distance between the crestal level and the widest diameter of the implant, as well as thicker gingival tissue. The greater the bone volume interproximally, the better it can maintain the papilla and bone at its desired level long-term.
This becomes important in narrower situations where either implants need to be placed close to each other, or the implant will be close to an adjacent natural tooth while still providing enough interproximal space for healthy bone and gingival maintenance. The post length between the top of the implant platform and the bottom of the widening of the abutment head is available in two lengths, short (0.5 mm) and long (2.0 mm) for crown and bridge applications.
This permits the implant to be placed at different depths subcrestally and have the restorative margin at the proper level.
The Bevel Hex connector has sloped shoulders below the hex functioning like an internal hex. This unique bevel allows the abutment to engage the crestal portion of the implant, taking stress off the abutment screw, thereby decreasing the potential for screw loosening and stress concentration on the abutment screw that may lead to screw fracture. When this connector option is planned, the implant can be placed subcrestally, crestally, and also can be set coronal to the crestal bone.
CLINICAL SITUATIONS
WHEN SUFFICIENT BONE IS PRESENT IN RIDGE HEIGHT AND WIDTH
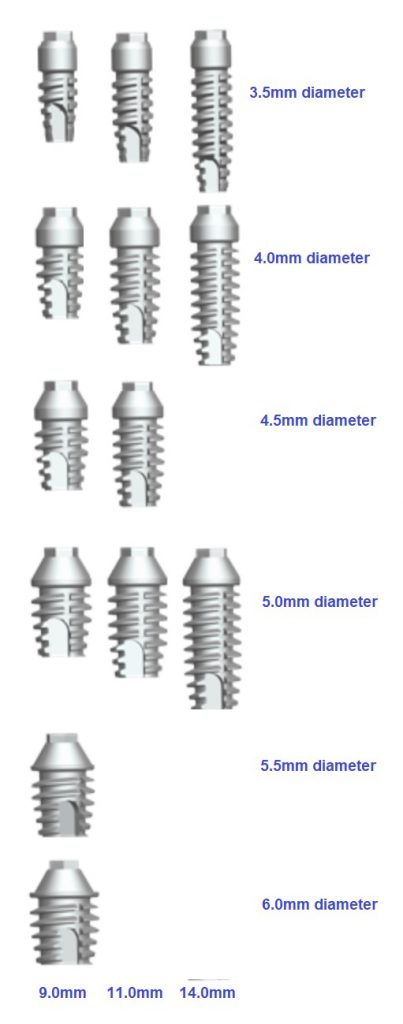
Sufficient bone is found in volume with the ridge presenting with adequate height, as well as buccal-lingual width to accommodate in the majority of clinical situations where implants are planned. When that is present, the Quantum Summa and Magnum implants are ideally suited for implant placement. These implants are available in widths of 3.5, 4.0, 4.5, 5.0, 5.5 and 6.0 mm with lengths of 8, 9, 11 and 14 mm (depending on the diameter). (Figure 4)
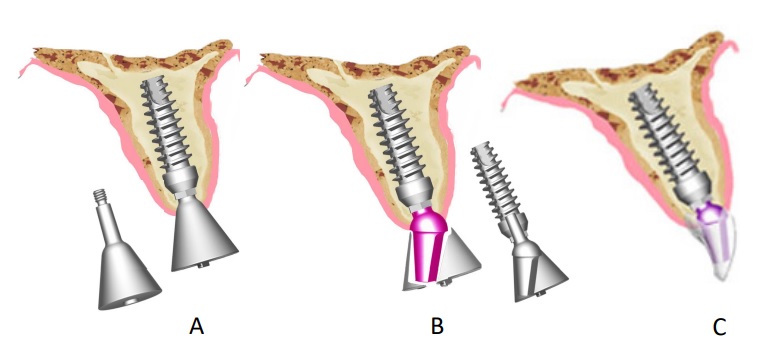
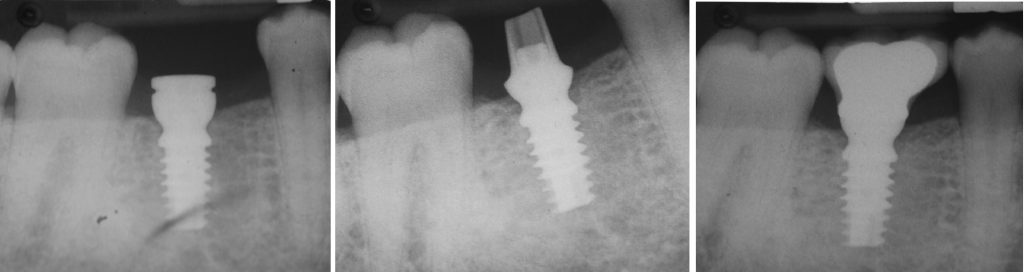
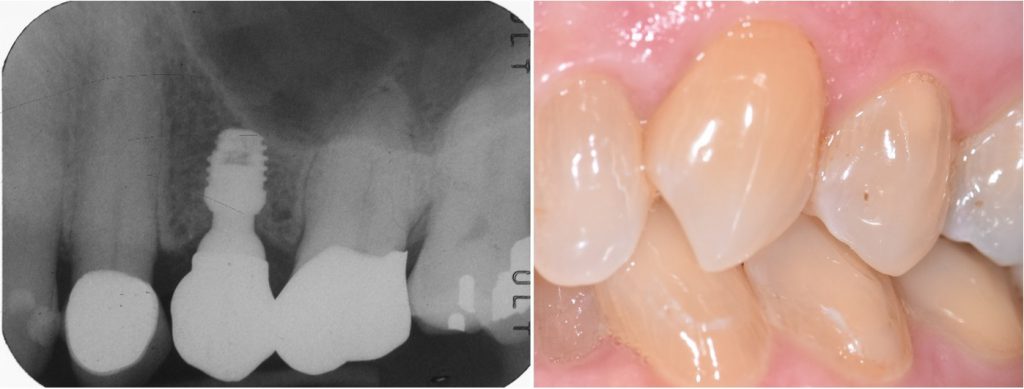
To expand options prosthetically and surgically, the Summa implant incorporates the 3-in-One connector at the platform, which allows modification of placement depth. Deeper placement depth may be utilized when treating the maxilla (Figure 5) or mandible (Figure 6) with the TaperLock or Taper Lock Threaded connection option.

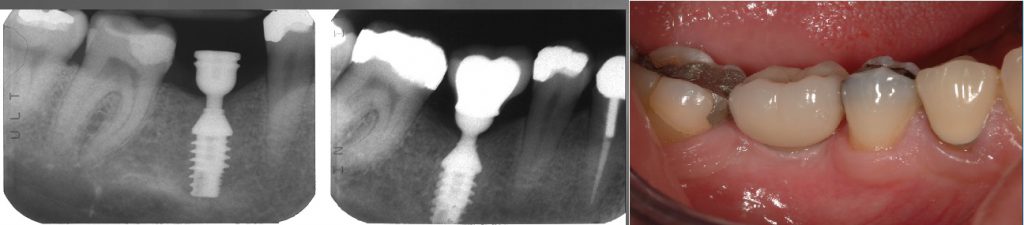
When utilizing the Hex connector option, the implant may be placed with the sloped shoulder at the crestal height or slightly below. (Figure 7)
Quantum allows for good placement stability in addition to ideal immediate placement, immediate fixation, and immediate loading.
INADEQUATE HEIGHT FOR IMPLANT PLACEMENT WITHOUT ADDITIONAL SURGICAL INTERVENTION
Ridge height decreases in an apical direction overtime, following tooth loss, when nothing is present in the ridge at that position. Atrophy of the bone results due to the lack of intraosseous stimulation. In the maxillary posterior, atrophy combined with enlargement of the maxillary sinus (a natural occurrence whether teeth are present or have been lost), creates potential challenges in placing implants in this region without supplemental sinus augmentation procedures to increase bony ridge height. In the mandibular arch, this may present a clinical challenge due to the inferior alveolar nerve (IAN) and what bone height is available crestal to that anatomical structure to accommodate implant placement.
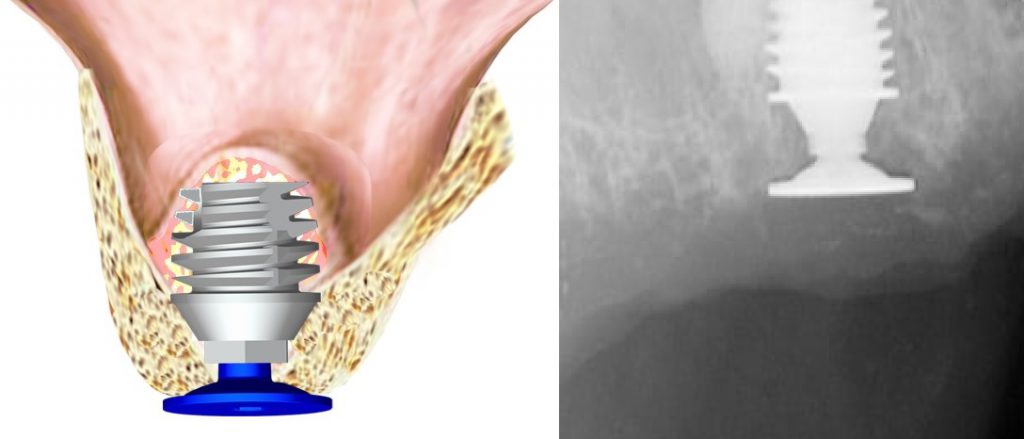
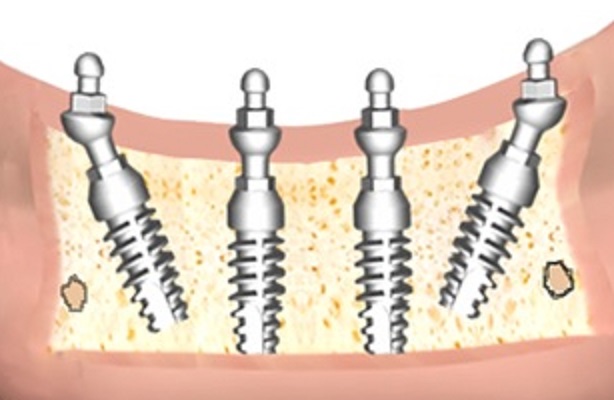
Short implants offer the advantage of allowing placement in decreased crestal height to avoid supplemental surgical procedures. The Quantum Short-T implant was designed in a 6mm height for those clinical situations. (Figure 8)

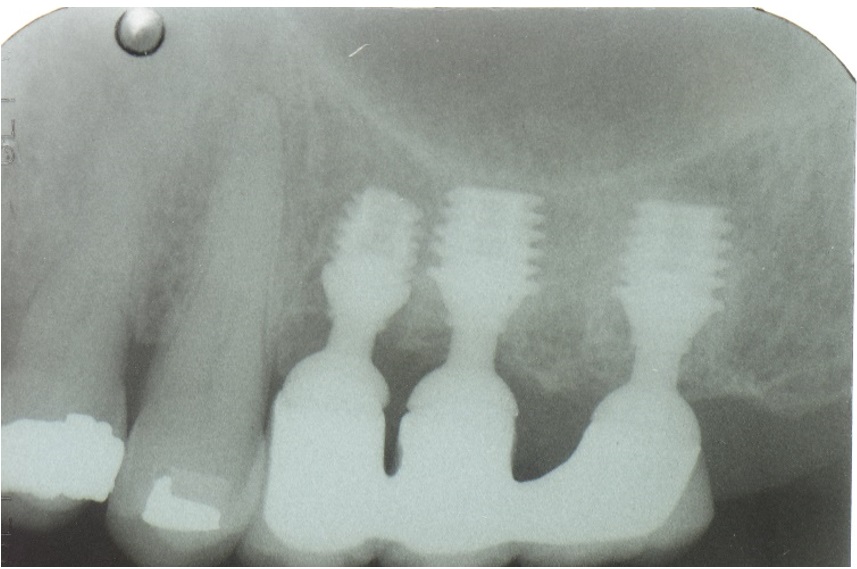
The implant is available in diameters from 4.0 to 6.0mm to accommodate various ridge widths present. Utilization in the posterior maxilla allows avoidance of the sinus (Figure 9) and in the posterior mandible avoids infringement on the IAN (Figure 10).

The Short-T implant is designed, same as the other Quantum implants, with three restorative platform abilities in the same implant, minimizing how many implants are needed to be stocked by the practitioner and allowing modification of surgical placement or prosthetics once the placement is initiated.
When placed so that the implant is flush with the crest, a 6mm depth of available bone is required. If greater height is available (up to 9mm), the Short-T may be placed subcrestal or if less height is present (4-6mm), it may be placed accordingly. (Figure 11)
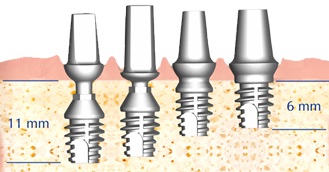
The ability to vary crestal depth placement also applies to the Summa and Slim implant lines increasing placement customization at surgery.
When sinus augmentation is indicated along with simultaneous implant placement, a wider Healing Plug is required in this clinical situation to prevent accidental displacement of the implant into the sinus. Utilization of a Morse Taper type connector on the healing abutment requires the abutment to be tapped into the implant and may displace the implant in a superior direction into the sinus. Quantum offers a Healing plug for Short-T, Slim, Summa, and Magnum that utilizes a Taper thread connector with a wide flat head so that healing plug placement does not require to be tapped, thus preventing accidental sinus displacement.
In addition, the flat head allows for soft tissue coverage at surgery. (Figure 12)
NARROW ARCH WIDTH
Limited width of ridge can present in either the mesial-distal or buccal-lingual dimension, related to resorption of the ridge or limited by the space between adjacent teeth. It is not unusual to have a narrow ridge mesial-distally in the maxillary lateral incisor or mandibular incisor positions, as those natural teeth are narrow in dimension that an implant would be replacing. Availability of a two-piece implant for these clinical situations permits the option of delayed loading when insertion torque has too low a value, or another clinical decision indicates that approach, or immediate loading with abutment angle alteration that a single-piece implant in narrow diameter will not permit.
The Slim implant is, as with other Quantum implants, available with three restorative platform abilities in the same implant. This allows the practitioner to place the implant subcrestal or slightly supracrestal and have different restorative options to accommodate various clinical situations.
The implant has a 3.0mm diameter with availability in 9.0, 11.0 and 14.0mm lengths. (Figure 13)
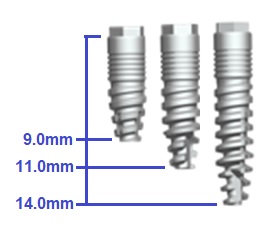
Ideally suited for those narrow clinical situations that are frequently found in the mandibular incisal positions where mesial-distal width may create a clinical challenge. (Figure 14)

HYBRIDS AND OVERDENTURE OPTIONS
Patients may require a hybrid or an overdenture approach for various reasons versus a fixed approach when treating the full arch. Those reasons may be easier home care when the prosthesis can be removed for cleaning by the patient, financial costs being lower for a removable approach, and the patient’s desire for improved denture retention over a fixed approach that may require more implants for a full arch.
An ideal option that can be utilized for either an overdenture or fixed detachable hybrid restoration is the Qfit abutment implant supported system providing a screwless, cementless attachment between the prosthesis and the implants.
When utilized with a fixed approach removal at hygiene, recall appointments is simplified and the patient can be trained to remove it for daily home care.
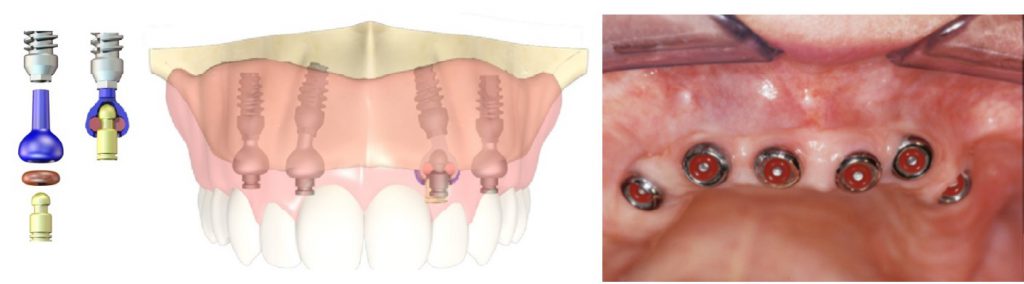
When extensive ridge resorbtion has occurred, flanges can be extended for esthetic purpose. The prosthetic design also allows elimination of all flanges and is well suited for those clinical situations where minimal ridge resorption has occurred, and maintenance of the residual ridge is desired. The Qfit abutments utilize the TaperLock connection and are available in 0°, 15°, and 25° to allow parallelism. The abutments are provided in short, regular, and long lengths to accommodate implant placement depth and tissue thickness.
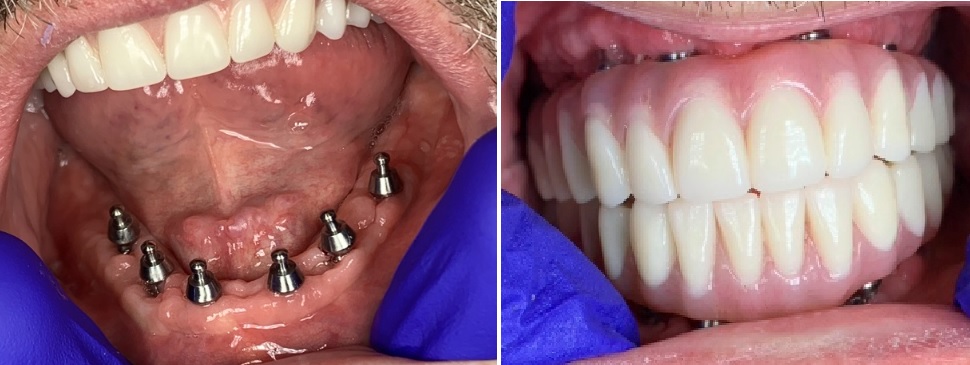
The retention coping is processed into the prosthesis either chairside or at the lab and houses an O-ring available in five retention levels. (Figure 15)
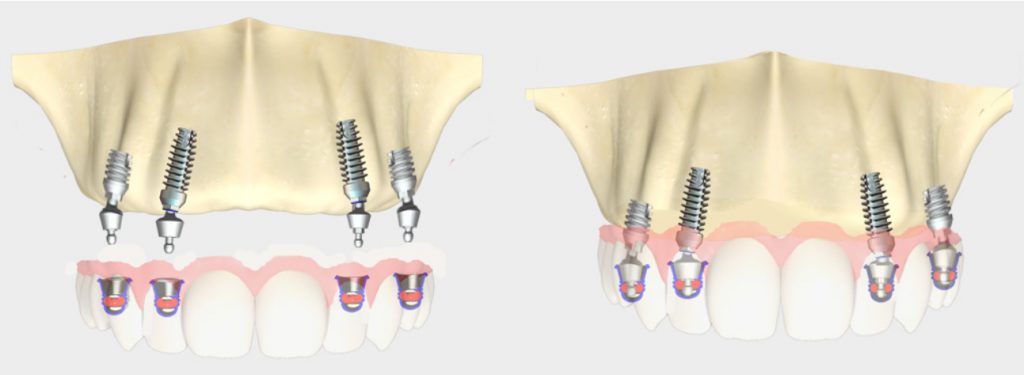
A fixed hybrid prosthesis results that can be removed when required. (Figure 16)
Should a metal reinforcement substructure be desired the copings can be processed to it then resin or ceramic added to the metal substructure as desired.
O-ring abutments are also available. These are offered in 0°, 15°, and 25° angulations with short, regular, and long post lengths. (Figure 17)
As this overdenture abutment utilizes the TaperLock connector, it can be rotationally positioned to obtain idea parallelism, then tapped into position to engage the Morse taper connector. The 25° greater angulation than other abutments available permit greater correction of the implants in the arch.
The maxillary anterior can present challenges related to the “triangle of bone,” which results in greater angulations when placing the implant than would be present in other parts of the arch. The Res-Q overdenture abutment system provides an option for treating those clinical situations with an overdenture. (Figure 18)
A low-profile tissue-level free-standing abutment is a solution for low vertical dimension clinical situations, which can compensate for up to 60° divergence between implants available in 0°, 15°, and 25° angulations. The retention post is processed into the overdenture decreasing the amount of vertical space required and its narrow dimension does not interfere with the dentures buccal flange allowing better esthetics, without the need to bulk out that area (Camel Look) of the overdenture to cover the attachments.
Insertion and removal of the overdenture is easy for the patient and a customizable level of retention is available with 5 different O-rings for a high degree of resiliency and tolerance.
WHEN WIDER MORSE TAPER CONNECTOR IS PREFERRED
Some practitioners may prefer a wider Morse taper connection and in those cases Magnum implants may be preferred.
This implant design has the Threaded fins to achieve stability at insertion and other features of the Quantum implants. It has an internal hex for engagement of the implant driver and a thread below the internal hex for the engagement of the Sinus Healing plug. (Figure 19)
Magnums are available in diameters of 4.5mm, 5.0mm, and 6.0mm, and lengths of 6mm, 8mm, and 11mm.
These implants are designed to be placed subcrestally or crestally, giving the practitioner greater surgical planning based on available bone present. (Figure 20)
CONCLUSION
Utilization of implants to replace missing teeth, whether single units or full arch, can present challenges related to the available bone present and its density. The threaded ‘fins’ on the Quantum implants provide stability at placement that permits immediate fixation and immediate loading compared to non-threaded press-fit finned implants.
This also decreases potential for accidental sinus displacement on insertion.
The unique platform on the 3-in-One connector allows modification on surgical placement, or the prosthetic plan, which increases flexibility during implant treatment.
For further information, please visit www.quantumimplants.com.
ABOUT THE AUTHORS

Dr. Raul R. Mena has a number of accomplishments to his name, including: Diplomate American Board of Oral Implantology Implant Dentistry, Medical College of Georgia, School of Dentistry, DMD, Oral, Cranio and Maxillofacial Implantology Hospital Residency, Cedars Hospital, Special Needs Dentistry Hospital Training, GRC Hospital, Bone Anchoring Hearing Aid, Cranio and Maxillofacial Implants Hospital Training, Misericordia Hospital, Chief Dental Technician, Medical College of Georgia, Crown and Bridge Rehabilitation Lab, Co-Director, Maxi-Residency Course, Pittsburgh University, School of Dental Medicine, and President, Quantum BioEngineering, LTD.

Dr. Gary E Chike graduated from the Medical College of Georgia with both a Master of Science degree in Medical Illustration, as well as a Doctorate in Dental Medicine. He maintains a full-time private practice in the suburbs of Atlanta, Georgia, and holds an adjunct faculty position at the Dental College of Georgia at Augusta University.

Dr. Rothenberg, a graduate of Tufts University Dental School in 1971, completed a 3 year CE implant program at Harvard School of Dental medicine in 1987. He has been practicing dentistry with a concentration in implantology in Marblehead, Massachusetts since 1971.

Dr. Kurtzman is in private general dental practice in Silver Spring, Maryland, a former Assistant Clinical Professor at University of Maryland in the department of Restorative Dentistry and Endodontics and a former AAID Implant Maxi-Course assistant program director at Howard University College of Dentistry.
He has lectured internationally on the topics of Restorative dentistry, Endodontics and Implant surgery and prosthetics, removable and fixed prosthetics, Periodontics and has over 770 published articles globally, several ebooks and textbook chapters.
Dr. Kurtzman has been honored to be included in the “Top Leaders in Continuing Education” by Dentistry Today annually since 2006.
He can be reached at [email protected].