



INTRODUCTION
It has been well-documented that the “triad” for success in endodontics includes instrumentation, irrigation, and obturation. Without proper instrumentation, effective irrigation and obturation become nearly impossible, as it is the instrumentation that facilitates adequate disinfection and then obturation. A delicate balance must be struck when instrumenting a canal. On the one hand, we must create sufficient space in the canal to accommodate irrigants and medicaments for proper disinfection. On the other hand, we must preserve radicular dentin to maintain the tooth’s structural integrity and its resistance to future fracturing. The goal of endodontics is not only to eliminate infection but also to ensure the tooth survives long-term. Proper instrumentation is essential in achieving these goals.
There has clearly been a revolution in the realm of instrumentation. The time is gone when one might spend countless visits hand instrumenting a root canal. Today, we have the most efficient systems, utilizing nickel titanium (NiTi) rotary files that allow for a relatively quick and seamless canal preparation compared to instrumentation with stainless steel hand files.1 As the saying goes, “with great power comes great responsibility,” and instrumentation with NiTi rotary systems is no exception. The dreaded file separation is something that anyone who has ever performed root canal therapy has experienced. The question is not how to deal with file separation but rather how to avoid it in the first place.
NiTi is a “superelastic” metallic alloy that, when flexed, undergoes an austenitic-martensitic transformation from its original structure, making it extremely flexible.2-5 This transformation usually happens when the metal is stressed, such as during the instrumentation of the root canal. If, however, the NiTi file is stressed beyond its elastic limit, it will break. One of the unique characteristics of NiTi is its “shape memory,” allowing it to be deformed during usage and then return to its original shape if it is not stressed beyond its elastic envelope.5 NiTi files also have high elastic flexibility in bending and torsion compared to stainless steel files. Flexibility is the hallmark of NiTi rotary files, and it is this feature that allows it to overcome one of the greatest challenges of root canal instrumentation, namely following the sharp and unexpected curves contained in most canals without causing iatrogenic damage, such as canal transportation—in essence, “respecting” canal anatomy (RCA) (Figures 1 and 2). Unfortunately, stainless steel files, in larger sizes, do not provide this same benefit. It is often forgotten that most canals have some curvature, whether in the mesiodistal dimension (noted radiographically) or buccolingually (not seen in 2D radiographs).6 When NiTi rotary files are used correctly, they are significantly faster and more efficient than stainless steel hand files.7-10
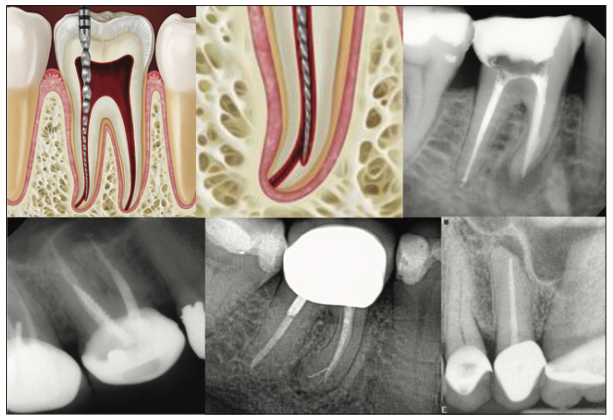
Figure 1. Altered apical anatomy: canal anatomy was not maintained due to increased dentin removal at the outer aspect of the curve caused by stiff files that often seek to return to their original shapes.
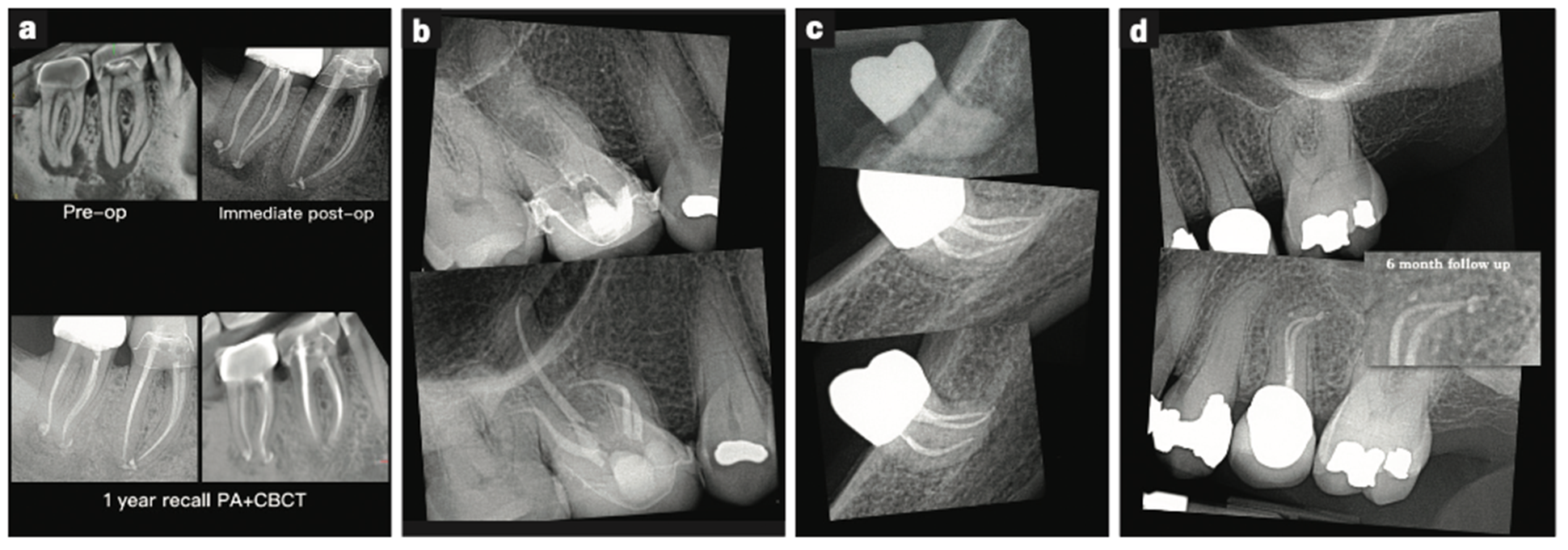
Figure 2. Cases that demonstrate “respecting root anatomy” via consistently maintaining canal curvatures.
Another unique feature of NiTi files is their tip design. When we think of a file, we think of an instrument that cuts along its entire length. Not so with most NiTi files, which have non-cutting tips that guide the instrument to the apical portion of the root canal. There is ample evidence that this feature makes NiTi superior in maintaining the original canal curvature, preserving the apical constriction, and avoiding canal transportation.11 When instrumenting a canal, one of 2 things will likely happen: You will accommodate the canal by following its complex and tortuous anatomy, or the canal will accommodate you by straightening itself out to accommodate your aggressive instrumentation. The process of instrumenting a canal will only be a successful endeavor when one learns to accommodate the canal and not vice versa.
During root canal preparation, our goal is to maintain the original canal anatomy and to avoid iatrogenic canal transportation. What follows are some tips to help navigate calcified and curved canals while avoiding the unfortunate file separation and/or iatrogenic damage to root structure. Avoiding these errors and “respecting” apical anatomy will lead to greater outcomes in our endodontic treatment.
TIP NO. 1: HAND FILES FIRST!
There was a time when instrumenting a canal was accomplished completely with hand files, which could take many visits. The pendulum has swung, and now with NiTi rotary instrumentation, endodontic treatment can be carried out more seamlessly in less time. There is the misconception, however, that rotary files have replaced hand files completely. This couldn’t be further from the truth. Many practitioners will try incorrectly to jump straight to rotary. It is important to remember that without first obtaining a smooth glide path to the apex with hand files, rotaries will be stressed beyond their elastic limits, leading to needless file separations. Hand filing a canal, as opposed to rotary instrumentation, provides tactile sensation, which allows one to better gauge the level of curvature and calcification. As a general rule, rotary files should never be placed in a canal before the canal has been properly “scouted” with hand files. If you can’t get a hand file to length in a canal, rest assured that if you then try to force a rotary into that same canal, the chances of separation and/or transportation are high.
TIP NO. 2: CORONAL FLARE
NiTi rotary instrument fractures can be greatly reduced by creating a proper coronal flare.12-14 This allows the unobstructed penetration by the hand file and then later the rotary file all the way to the working length. This is done by preflaring the canal orifice with a NiTi orifice opener, which is placed only in the coronal third of the canal. Most rotary systems will contain an orifice opener (Figure 3a). The benefit of this file is its short length and wider taper. This is also one of the goals of the “crown-down” instrumentation technique. By removing coronal interferences and restrictive dentin from the coronal third of the canal, one will have a much easier time placing both hand files and rotary files into the canal and then down to length. The orifice opener eliminates the “triangle of dentin,” which obstructs the orifice (Figure 4). You may successfully leave this triangle of dentin and negotiate around it, but this puts tension on the file at the occlusal end, making it more likely to separate should it find additional tension when negotiating an apical curve. The ProTaper S1 file (Dentsply Sirona Endodontics) (Figure 3b) is another great favorite of many endodontists for flaring the coronal and middle thirds of the root canal.
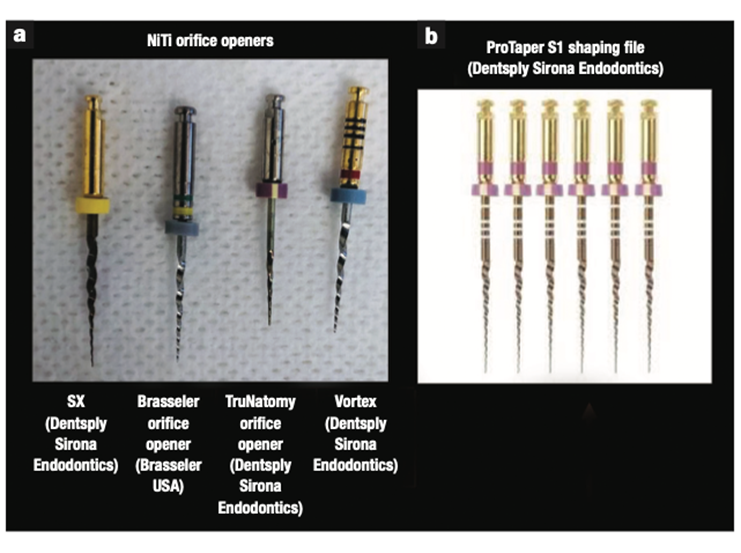
Figure 3. (a) Orifice openers and (b) shaping file.
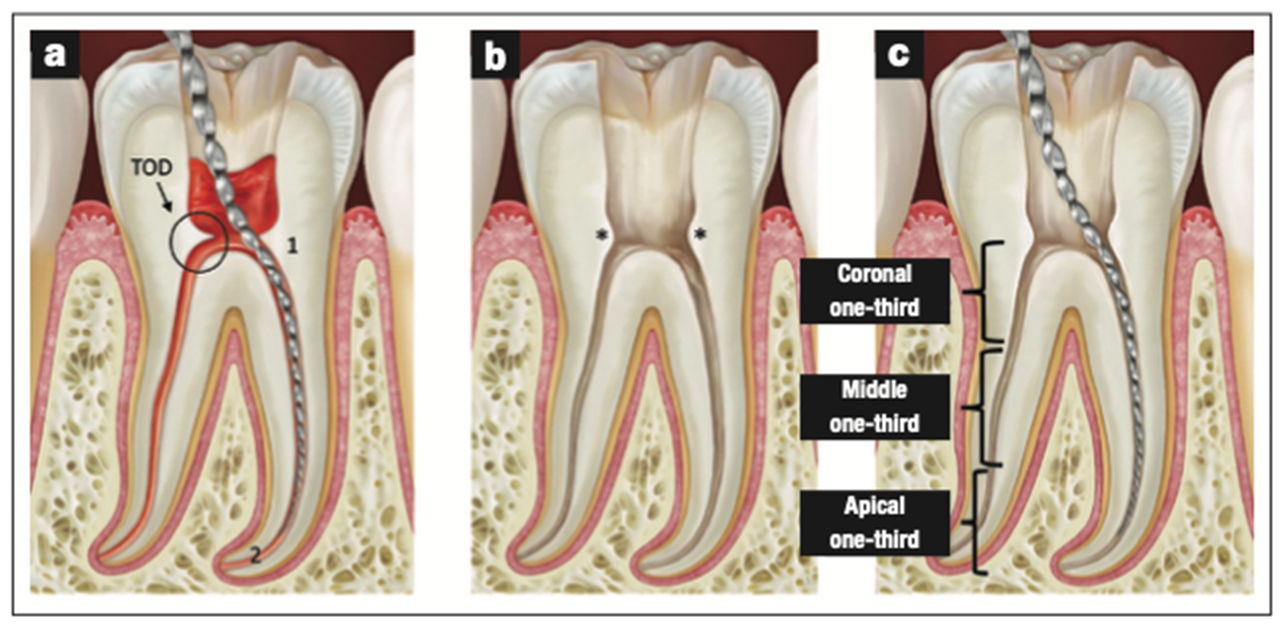
Figure 4. (a) “Triangle of dentin” obstructing entry into the root canal—the file is strained from navigating 2 curves instead of one. (b) The triangle of dentin is removed once the canal is coronally flared. (c) Unobstructed penetration of the file into the canal orifice and then the entire root canal system.
This file has the benefit of having a very narrow tip with a taper that allows for proper shaping of the coronal and middle thirds of the canal. It is prudent to remember that these rotary files should only be used after the canal has first been scouted with hand files. It is always important to stress moderation, as “over-flaring” a canal can weaken the tooth by removing too much dentin in critical zones, so while flaring is beneficial for many reasons, it should be done as conservatively as possible to avoid removing too much dentin, thereby weakening the root. The TruNatomy orifice opener (Dentsply Sirona Endodontics) (Figure 3a) is a great example of a file that appropriately flares the canal orifice without excessively removing dentin from the critical zones. One of the most important components for long-term tooth survival is maintaining as much dentin as possible, specifically pericervical dentin (PCD), which is the dentin near the alveolar crest (Figure 5). Preserving the dentin above and below the canal orifice/alveolar crest is crucial for long-term survival of the tooth.15,16
TIP NO. 3: GLIDE PATH
Another important component in proper instrumentation is establishing a glide path, which is the creation of a predictable path so that the rotary file can reach all the way to the working length unencumbered. The first step in creating this glide path is by hand filing the canal to at least a size 15 hand (K-) file. Although it is possible to skip the size 15 in loose canals, a tight canal will not accept a rotary file well before it has been opened to at least a size 15 K-file. Before one ever places a rotary file to length in a canal, he or she should first instrument the canal comfortably with an 8, a 10, and a 15 hand file to help remove the restrictive dentin and allow for a more predictable glide path. The orifice opener or ProTaper S1 can also help to establish this glide path. While most endodontists use K-files for hand instrumentation, a much stiffer C or C+ file can also help to loosen up a tight canal, as smaller size K-files will often buckle when encountering a tight canal. The use of these hand files will, in essence, pave the pathway for the first rotary instrument to length and reduce the chance of separation of the rotary files. Establishing the glide path also causes less canal transportation (“ledging”) as compared to preparations done without a glide path. To quote Dr. Cliff Ruddle, “Whoever owns the glide path wins the shaping game of endodontics.”
TIP NO. 4: SEQUENCE MATTERS!
Don’t skip around. If you start with a size 8 file, don’t skip to a size 15 as your next file in the canal. While this might be okay in a looser canal, developing healthy habits while instrumenting is important. It is tempting to cut corners, especially when hand filing a canal, as this can be quite tedious. This will place more stress on the larger size files and increase the odds of instrumentation errors, such as canal blockage and/or ledging (Figure 1).
TIP NO. 5: RECAPITULATION
After each use of a rotary file, make sure to re-enter the canal with a smaller hand file. Rotary instrumentation creates a significant amount of debris, which can clog up the canal, negatively affecting the ever-important glide path. What occasionally happens is that, at some point during the instrumentation process, your file no longer reaches the working length. This is because either the canal has been ledged or, more commonly, dentinal debris has clogged a portion of the canal. Re-entering with smaller files throughout the instrumentation process to break up this debris allows for maintenance of the glide path. Putting a slight bend on the tip of the hand file can also help work around a blockage. Trying to penetrate this blockage with a rotary file will inevitably lead to file separation. Without the glide path, we end up stressing (pushing too hard on) the NiTi files, ultimately leading to fracture.
TIP NO. 6: REUSE OF NICKEL TITANIUM FILES
How many times is too many? File fatigue will depend on several variables, including instrument properties, canal morphology, and operator skills.17 For example, working one calcified canal will stress a file more than working multiple “loose” canals. Forcing a file in a tight or curved canal will fatigue it more than placing a file in a relatively straight and loose canal. Thus, there is no magic number of times a file can be used. It is prudent to often examine the cutting edges for wear and strains.
TIP NO. 7: ROTARY MOVEMENTS
Stopping the rotary file midway down a canal will put more pressure and stress on the file, predisposing it to fracturing because of cyclic fatigue. Constant movement of the rotary file within the canal will better distribute the forces and prevent breakage. The rotary file should be in motion as it is removed from the canal. Stopping the motor while the file is in the canal can potentially cause the file to get locked into a tight spot and separate.18-25 A rotary file should be used in an “in-and-out” (pecking) motion with light apical pressure. Never force a rotary file into a canal, and never place heavy apical pressure as this will cause the file to lock into the canal and separate. When NiTi files fracture, it is due to cyclic fatigue or torsional strain. Torsional fracture is when the tip of the instrument locks in a canal while the shaft continues to rotate. Excessive force on the file during instrumentation causes the tip of the file to lock in a “tight spot.” Larger-sized files tend to be more resistant to these torsional fractures as they don’t bind as easily. Cyclic fatigue occurs after the repeated bending of instruments in curved canals, causing the metal to fatigue and fracture. Obviously, the more curved a canal is, the higher the probability of the file separating due to cyclic fatigue.
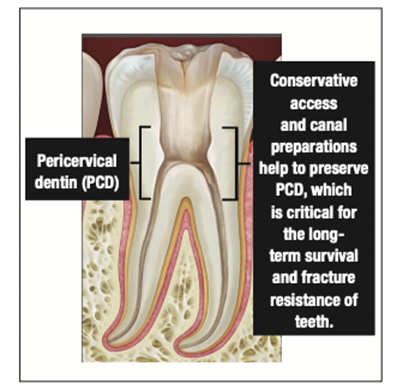
Figure 5. Preserving the dentin above and below the canal orifice/alveolar crest is crucial for long-term survival of the tooth.
TIP NO. 8: FILE INSPECTION
One of the indicators that a file has been fatigued and is on the cusp of breakage is when the flutes of that file begin to unwind. It should be a habit to always inspect the file for this unwinding, and when you see it, toss it (Figure 6). File inspection should also include wiping the file of debris before re-entering the canal. This can be done with wet cotton gauze.
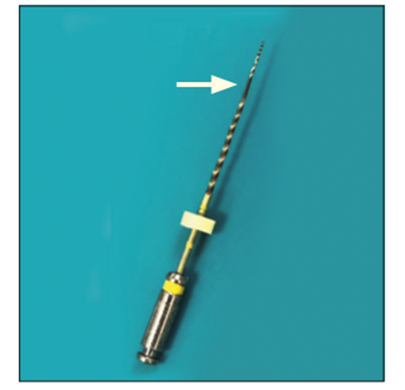
Figure 6. Note file deformation (unwinding of file flutes). This is an indicator that the file is on the cusp of breakage and should be discarded.
TIP NO. 9: IRRIGATION AND LUBRICATION
Never file a dry canal as this will create excessive debris in the canal, which ultimately will lead to canal blockage. In trying to force your way through a blockage, the chances of file separation are significantly increased. Irrigation serves the purpose of disinfection and flushing of debris from the canal. Some commonly used lubricants/irrigants are RC prep (Premier Dental), EDTA, sodium hypochlorite, Triton (Brasseler USA), QMix (Dentsply Sirona), and MTAD.
TIP NO. 10: STRAIGHT-LINE ACCESS
Straight-line access into the pulp chamber as well as the root canal is crucial to help avoid coronal tension on the file.26 There are 2 components to straight-line access: the initial access into the pulp chamber and the access into the root canal. Managing both well puts less stress on the file and will ultimately prevent needless file separation. This also aids in glide path maintenance. It is prudent to point out that while straight-line access into both the pulp chamber and root canal is important, we must also strive to preserve as much dentin as possible to avoid weakening the tooth. Many have the motto “You can’t do what you can’t see,” but with more experience, skill, magnification, and image guidance, one can create smaller access preparations and still avoid iatrogenic damage while locating and treating all the complexities of the root canal system. The great benefit to conservative access is preserving the very valuable PCD (Figure 5).
TIP NO. 11: BITE BLOCK
Having the patient use a bite block during treatment is another great way to avoid file separation. When the patient’s range of opening is compromised, your access to the posterior teeth may be limited. A sudden closure, even slight, by the patient during instrumentation can lead to file fracture.
TIP NO. 12: PRE-BEND!
Obtaining access into a canal with hand or rotary files can be difficult, especially in an MB canal of a maxillary molar or a mesial canal of a lower molar. The angulation and location of the canal can make it challenging, especially with longer-length rotary files. A good piece of advice is to use shorter length files in these situations (21-mm length as opposed to 25-mm or 31-mm). One of the benefits of NiTi files is that they can be pre-bent to obtain the proper angulation. Putting a curve on the file can simplify this complexity (Figures 7a and 7b). Coronal flaring with shorter length files also helps obtain better access and prevents the dreaded “snap” of the file when it’s improperly placed in the canal. Pre-bending the tip of a small hand file also helps to navigate the curvatures within the canal itself and can help work around a blockage or ledge (Figure 7c).
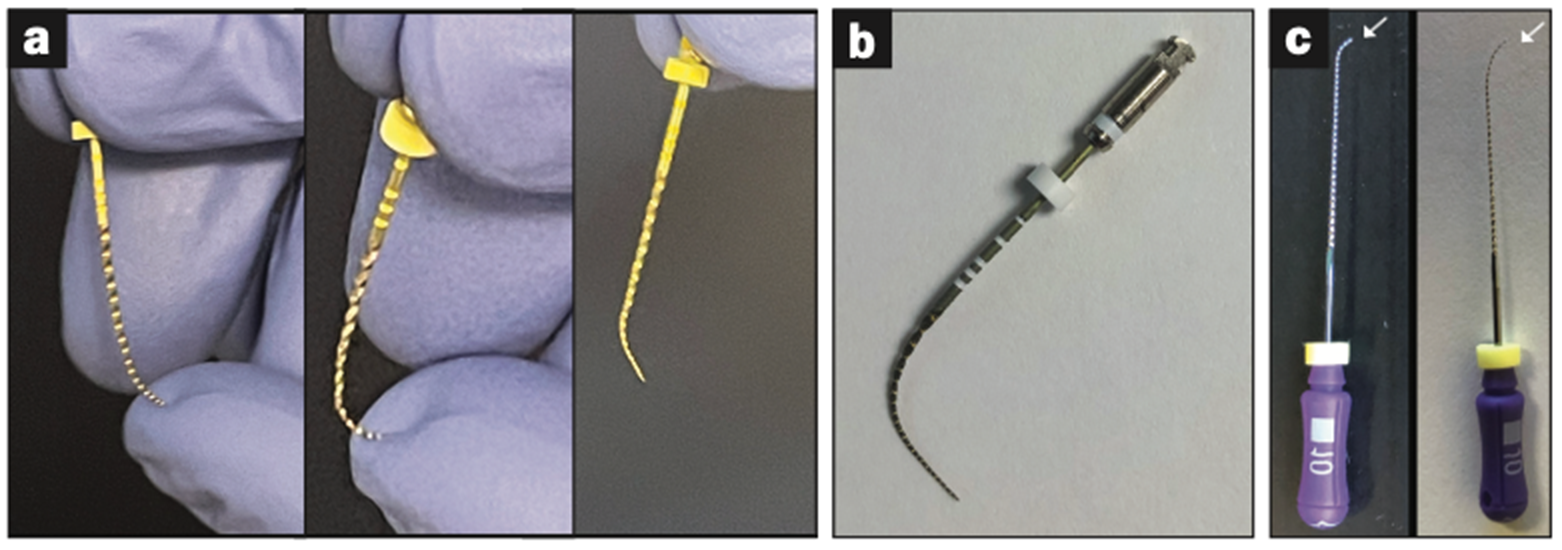
Figure 7. Pre-bending the tip of a small hand file can help to navigate curvatures within the canal itself and help work around a blockage or ledge.
TIP NO. 13: BE PREPARED!
Thoroughly inspect the radiograph before starting a case. CBCT can also help to evaluate subtle canal curvatures. Extra care in rotary file usage will be needed in cases that have calcified or curved roots. Never rush! Never blame the file! Never cut corners! With proper technique, patience, and experience, separating files will become a rare occurrence, and navigating curved and calcified canals will become less stressful and easier to manage.
ACKNOWLEDGMENTS
The author wishes to thank Drs. Charles Solomon, Leslie Elfenbein, and Eric Wachs for their valuable input and guidance.
REFERENCES
1. Short JA, Morgan LA, Baumgartner JC. A comparison of canal centering ability of four instrumentation techniques. J Endod. 1997;23(8):503–7. doi:10.1016/S0099-2399(97)80310-X
2. Peters OA, Paque F. Current developments in rotary root canal instrument technology and clinical use: a review. Quintessence Int. 2010;41(6):479–88.
3. Viana AC, Chaves Craveiro de Melo M, Guiomar de Azevedo Bahia M, et al. Relationship between flexibility and physical, chemical, and geometric characteristics of rotary nickel-titanium instruments. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110(4):527–33. doi:10.1016/j.tripleo.2010.05.006
4. Peters OA, Gluskin AK, Weiss RA, et al. An in vitro assessment of the physical properties of novel Hyflex nickel-titanium rotary instruments. Int Endod J. 2012;45(11):1027–34. doi:10.1111/j.1365-2591.2012.02067.x
5. Shen Y, Zhou HM, Zheng YF, et al. Metallurgical characterization of controlled memory wire nickel-titanium rotary instruments. J Endod. 2011;37(11):1566–71. doi:10.1016/j.joen.2011.08.005
6. Cunningham CJ, Senia ES. A three-dimensional study of canal curvatures in the mesial roots of mandibular molars. J Endod. 1992;18(6):294-300. doi:10.1016/s0099-2399(06)80957-x
7. Kazemi RB, Stenman E, Spångberg LS. A comparison of stainless steel and nickel-titanium H-type instruments of identical design: torsional and bending tests. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;90(4):500–6. doi:10.1067/moe.2000.108959
8. Schäfer E, Tepel J, Hoppe W. Properties of endodontic hand instruments used in rotary motion. Part 2. Instrumentation of curved canals. J Endod. 1995;21(10):493–7. doi:10.1016/s0099-2399(06)80519-4
9. Tepel J, Schäfer E, Hoppe W. Properties of endodontic hand instruments used in rotary motion. Part 3. Resistance to bending and fracture. J Endod. 1997;23(3):141–5. doi:10.1016/S0099-2399(97)80262-2
10. Tepel J, Schäfer E. Endodontic hand instruments: cutting efficiency, instrumentation of curved canals, bending and torsional properties. Endod Dent Traumatol. 1997;13(5):201-10. doi:10.1111/j.1600-9657.1997.tb00041.x
11. Kuhn WG, Carnes DL Jr, Clement DJ, et al. Effect of tip design of nickel-titanium and stainless steel files on root canal preparation. J Endod. 1997;23(12):735–8. doi:10.1016/S0099-2399(97)80345-7
12. Hartmann RC, Peters OA, de Figueiredo JAP, et al. Association of manual or engine-driven glide path preparation with canal centring and apical transportation: a systematic review. Int Endod J. 2018;51(11):1239–52. doi:10.1111/iej.12943
13. Kwak SW, Ha JH, Cheung GS, et al. Effect of the glide path establishment on the torque generation to the files during instrumentation: an in vitro measurement. J Endod. 2018;44(3):496-500. doi:10.1016/j.joen.2017.09.016
14. Patiño PV, Biedma BM, Liébana CR, et al. The influence of a manual glide path on the separation rate of NiTi rotary instruments. J Endod. 2005;31(2):114–6. doi:10.1097/01.don.0000136209.28647.13
15. Clark D, Khademi J. Modern molar endodontic access and directed dentin conservation. Dent Clin North Am. 2010;54(2):249–73. doi:10.1016/j.cden.2010.01.001
16. Clark D, Khademi JA. Case studies in modern molar endodontic access and directed dentin conservation. Dent Clin North Am. 2010;54(2):275–89. doi:10.1016/j.cden.2010.01.003
17. Yared G, Kulkarni GK. An in vitro study of the torsional properties of new and used rotary nickel-titanium files in plastic blocks. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96(4):466–71. doi:10.1016/s1079-2104(02)91706-3
18. Miyai K, Ebihara A, Hayashi Y, et al. Influence of phase transformation on the torsional and bending properties of nickel-titanium rotary endodontic instruments. Int Endod J. 2006;39(2):119–26. doi:10.1111/j.1365-2591.2006.01055.x
19. Wolcott J, Himel VT. Torsional properties of nickel-titanium versus stainless steel endodontic files. J Endod. 1997;23(4):217–20. doi:10.1016/S0099-2399(97)80049-0
20. Walia HM, Brantley WA, Gerstein H. An initial investigation of the bending and torsional properties of Nitinol root canal files. J Endod. 1988;14(7):346–51. doi:10.1016/s0099-2399(88)80196-1
21. Parashos P, Messer HH. Rotary NiTi instrument fracture and its consequences. J Endod. 2006;32(11):1031–43. doi:10.1016/j.joen.2006.06.008
22. Plotino G, Grande NM, Cordaro M, et al. A review of cyclic fatigue testing of nickel-titanium rotary instruments. J Endod. 2009;35(11):1469–76. doi:10.1016/j.joen.2009.06.015
23. Bergmans L, Van Cleynenbreugel J, Wevers M, et al. Mechanical root canal preparation with NiTi rotary instruments: rationale, performance and safety. Status report for the American Journal of Dentistry. Am J Dent. 2001;14(5):324–33.
24. Sattapan B, Nervo GJ, Palamara JE, et al. Defects in rotary nickel-titanium files after clinical use. J Endod. 2000;26(3):161–5. doi:10.1097/00004770-200003000-00008
25. Pruett JP, Clement DJ, Carnes DL Jr. Cyclic fatigue testing of nickel-titanium endodontic instruments. J Endod. 1997;23(2):77-85. doi:10.1016/S0099-2399(97)80250-6
26. Patel S, Rhodes J. A practical guide to endodontic access cavity preparation in molar teeth. Br Dent J. 2007;203(3):133–40. doi:10.1038/bdj.2007.682
ABOUT THE AUTHOR
Dr. Stern is a Diplomate of the American Board of Endodontics. He is the director of endodontics at the Touro College of Dental Medicine and frequently lectures on the subject of clinical endodontics. He has lectured at many local county dental societies, at the New Jersey Dental Association Annual Session in May 2019, and at the Greater New York Dental Meeting in 2020. He maintains a private practice, Clifton Endodontics, in Clifton, NJ.
He can be reached at jstern5819@gmail.com or via the Instagram handle @the_barbed_broach1.
Disclosure: Dr. Stern reports no disclosures.








