
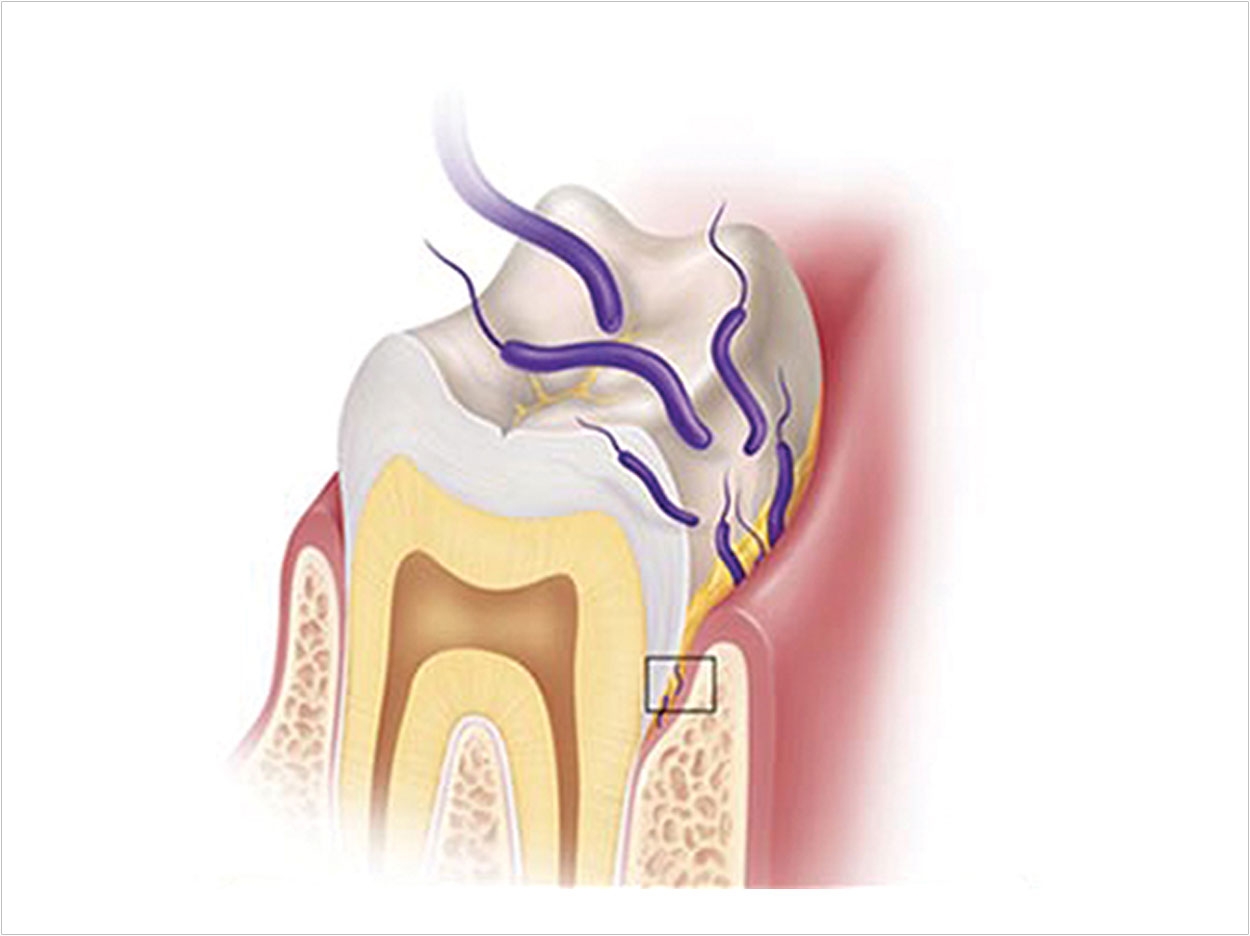
Dental caries and periodontal disease are transmittable bacterial infections of the teeth and gums.1,2 Each infection has unique characteristics, yet both share the common source of infection—oral biofilms (Figure 1). Both diseases have been implicated as inflammatory diseases.3,4 Inflammatory diseases affect our systemic health and contribute to the aging process.5,6 Incidence of dental caries and periodontal disease are both rising.7,8 Despite these compelling facts, motivating patients to seek treatment for painless pathology can be frustrating. Clinicians can benefit by using additional ways to detect, reveal, and oblige our patients to treatment.
Use of disclosing dyes have a mainstay for revealing biofilm accumulation, but this is a messy and “old fashioned” process. There are several new technologies appearing in the market, improving our ability to detect biofilm, inflammation, and dental caries. One company, ACTEON North America, has developed a high-performance intraoral camera (SoproCARE) that can highlight dental plaque, gingival inflammation, and effectively assists in enamo-dentinal caries detection (Figure 2). This camera can connect to any image management program and is easy for the dentist and hygienist to use. Intraoral cameras have been used for years to communicate various clinical situations. We have been involved in the clinical use of this fluorescence light-induced camera used for evaluation of biofilm, caries, and gingival inflammation.
This article will describe a protocol we have developed for daily use of this technology during the prophylaxis appointment.
THE PREMISE
Treatment acceptance is no longer just based on relationship building skills. Most patients enjoy a trusting relationship with dental offices and engage in prevention through prophylactic “check-up” visits. Yet many people’s behavior has changed as their culture has changed. Fifty seven percent of people say they talk more online than they do in real life (in households with income of $75k or more).9 Even when personal recommendations are made, online research cements the decision for service providers and purchase decisions. This is the digital age.
In order to best serve our patients, it is important that you develop a comprehensive, integrated, user-friendly platform to facilitate communication and address patient preferences. The visual communication provided by an intraoral camera fits into this digital consciousness.
THE TECHNOLOGY: FLUORESCENCE
The SoproCARE intraoral camera is a high-quality, high-magnification camera (up to 110x) that uses white and blue LEDs projected into the oral tissues and biofilm which is then absorbed and reflected back in the form of fluorescence. Dental tissues have fluorescent molecules that absorb light, and then emit the energy back as fluorescent light. This is called autofluorescence.10 The device uses selective chromatic amplification of the fluorescent chroma to reveal caries, calcified and noncalcified dental plaque, and gingival inflammation.
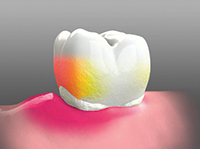
The camera is unique in that it has 3 modes. It has a Daylight mode for natural high quality image of the tissues, a CARIO mode that uses the blue light to amplify the fluorescent chroma for visual detection of dental caries, and a PERIO mode that combines the blue and white lights to highlight any biofilm and inflammation that may be present (Figures 3 and 4).
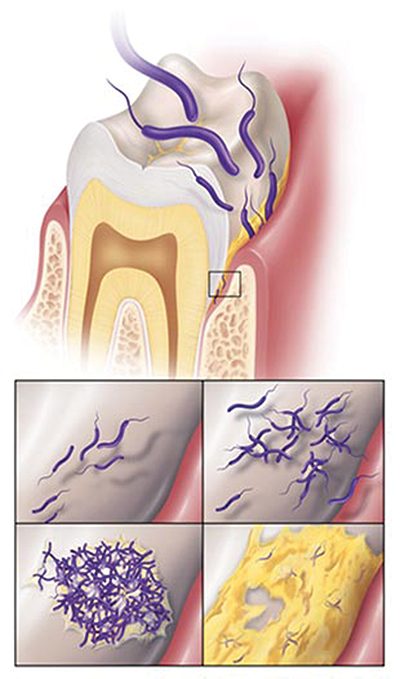 |
| Figure 1. Dental caries and periodontal disease are biofilm induced. |
 |
| Figure 2. SoproCARE intraoral camera (ACTEON North America). |
 |
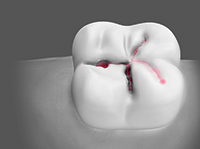 |
| Figure 3. PERIO mode. Schematic illustration of the colors produced: at the neck, white indictes soft deposits; above that, orange indictes calcified deposits and tartar; and on the gum, red indictes inflamed areas. | Figure 4. CARIO mode. Schematic illustration of the colors produced: the areas warning of carious activity appear red. |
It is now possible to layer, upon the high quality intraoral pictures, a graphic color interpretation of what these conditions mean to the patient with regard to home care, cavities, and periodontal inflammation.
What remains to be discussed is a system to implement the process.
THE IMPLEMENTATION PROTOCOL
It starts with an auxiliary driven (nonthreatening personnel) approach—“Mrs. Smith, the doctor asked me to take a preliminary look in your mouth for any potential problem areas. We are now using the latest technology for early detection of cavities and gum disease. This report card is a color-coded guide to rating your risk. We want you to be involved in decisions about your own health, so we will be showing you and telling you what we see as we go along. Let’s get started!”
Use the SoproCARE camera in the Daylight mode. Start with the teeth first (cavities are still king). Identify stained fissures, cracks in teeth, or restorations and wear. Then switch the camera over to the CARIO mode to grade if the lesions identified are carious. Finally, use the PERIO mode to view existing biofilm, mature biofilm (calculus), and any tissue inflammation.
Follow this with the doctor’s examination—The exam should not begin with, “Are you having any problems?” The hygienist or assistant has already done this. Instead, greet the patient and turn to the hygienist/assistant and ask, “Please bring me up to date. What are your findings?”
The hygienist/assistant should brief the doctor—on medical history/blood pressure. Remember that caries and periodontal pathology affect systemic health, and the examination should reflect this relevance!
Patient concerns—The periodontal condition and recommendations. “No pockets over 3 mm other than x. Areas still in need of attention. Last scaling.”
Recall/home care—“I recommended Mrs. Smith come back in 3 months.”
Today I noted these findings with the SoproCARE Display the images from the Daylight, CARIO, and PERIO modes.
Previous recommendations: “
I noted in the chart you are concerned about tooth No. 4 [you will have that image]. It looks like if that continues to be a problem, and we’d likely recommend a crown, but we’ll see.”
Review radiographic data, cosmetic issues, bite/wear, etc.
After a few repetitions of this suggested protocol, you will find it to be an efficient, comprehensive, codiscovery experience that supports the concepts of oral-systemic health, preventative health, and early disease detection.
APPLICATIONS
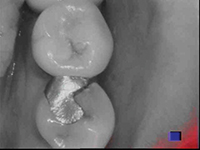
Communication—The intraoral camera is the fastest, most effective way to communicate to patients their oral status. The projection of intraoral images on to a large screen monitor fosters patients through the codiscovery process. We know that most dental treatment starts out asymptomatic, so a picture of a painless, fractured restoration helps the patient (and dental team) in the treatment decision process (Figure 5).
 |
 |
| Figure 5. Intraoral view, in CARIO mode, of a fractured restoration. | Figure 6. Pre-op view in Daylight mode at the start of check-up visit. |
 |
 |
| Figure 7. Pre-op view in PERIO mode. | Figure 8. Post-op view in Daylight mode confirming effectiveness and value of the prophylaxis appointment. |
 |
 |
| Figure 9. Pre-op view (upper left) of biofilm and apparent stain in Daylight mode. | Figure 10. View (same as Figure 9) in PERIO mode. Soft bacterial deposits are white, calcified deposits are orange-yellow, inflamed tissues are purplish-pink-red. |
 |
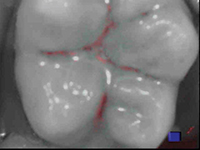 |
| Figure 11. View of suspicious grooves in magnified Daylight mode. Caries present? | Figure 12. The biofilm is removed from the occlusal grooves with air polishing to complete the evaluation; caries are red (CARIO mode). |
 |
 |
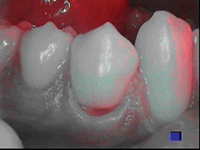
| Figure 13. A cervical lesion may be treated in a variety of approaches; the presence of red (indicating caries) aids in the treatment decision. | Figure 14. View of marginal ridge fracture unapparent to the patient, as seen during the examination process. |
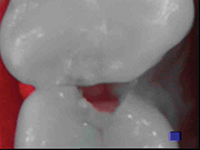 |
| Figure 15. Quick shift to CARIO mode indicates the presence of an active lesion. |
Home care evaluation; presence of biofilm—The prophylaxis appointment is the portal to patient education and motivation. With the continuing discoveries of interrelationships between oral and systemic disease, the dental team needs to present a meaningful depiction of the patient’s oral health status. If inflammation is the common mechanism connecting periodontal disease and cardiovascular disease, a picture of the oral biofilm with adjacent tissue inflammation can be a compelling way to communicate the importance of tissue management and homecare. High magnification as well as selective chromatic amplification also allow the clinician to evaluate the successful removal of deposits (Figures 6 to 10).
EARLY LESION DETECTION AND LESION EVALUATION
Light-induced fluorescence facilitates earlier caries lesion detection and subsequent less invasive treatment.11 In the protocol presented, the patient is alerted to the presence of caries by referring to the risk assessment card indicating dental caries as red in color with the SoproCARE device. Suspicious grooves can be evaluated as to the need for preventive treatment such as sealants versus more invasive preparation (Figures 11 and 12). The status of cervical lesions can be evaluated to determine the course treatment—preparation versus fluoride varnish, remineralizing pastes, etc (Figure 13). Proximal fractures can be evaluated as to the presence of active caries in real time as the patient sees the clinical conditions as the dentist or auxiliary conducts the examination (Figures 14 and 15).
| Our Experience With SoproCARE Technology Joann “Jodi” Papanier, RDH, LLA Have you ever been “on the fence” during a dental examination with a new or existing patient at your dental practice? At our dental practice, The Dental Healthcare Group, we are not in the habit of saying, “Let’s just put a watch on this tooth and check it again in a few months,” or “Let’s just watch your gums and see if the bleeding subsides by the time you are due to come back for your next cleaning.” All of our patients receive a complete diagnosis and a comprehensive treatment plan. Our goal is to deliver optimal treatment plans so our patients can make fully informed and knowledgeable decisions regarding their dental health and their overall health. In our opinion, there are 4 critical steps to successfully achieving patient compliance and acceptance of dental treatment: communication, comprehension, diagnosis, and treatment planning. In order to adhere to our goal of delivering optimal treatment planning, we rely heavily on utilizing accurate tools both at the chair and in our consultation room. The SoproCARE intraoral camera (ACTEON North America) has become a necessary aid in our office. This instrument is fast and easy to operate, and the level of accuracy (compared to other intraoral cameras) is Although maintaining the health of hard tissue (teeth, bone, etc) is of significant importance, as hygienists, Beverly and I obviously make it our priority to pay close and specific attention to the soft tissue (gingiva, mucosa, etc). With the regular and repeated use of the SoproCARE intraoral camera, Beverly and I have made charting and following the pattern of inflammation a mandatory protocol for every visit for all of our patients. Most importantly, these findings and patterns of inflammation are documented and kept on file for review for future comparisons. Without the use of this technology, we would not be able to follow and diagnose the periodontal status of our patients with such accuracy, certainty, and confidence. When comparing the SoproCARE camera with other intraoral cameras, I have experienced and discovered false caries detection and inaccurate levels of inflammation with the others. This can occur especially if a patient has not had a recent and complete oral hygiene cleaning immediately prior to using other intraoral cameras. The SoproCARE intraoral camera has a more sophisticated accuracy that limits this false detection from occurring simply due to an unclean mouth. Get “off the fence” during your dental examinations! Make it your personal challenge to deliver optimal treatment plans to all of your patients. In our opinion, based on our clinical experiences, this would not be achievable without SoproCARE intraoral camera technology. |
IN SUMMARY
The days of handing patients a mirror to show their oral health status are long gone. Intraoral cameras (such as SoproCARE), used with the suggested protocol outlined in this article, facilitate the codiscovery process through technology which is “cognitively familiar” to today’s digitally aware dental patients.
Doctor-patient communication is streamlined, and patient education and motivation is facilitated with this protocol. In addition, early detection of caries and inflammation is also made possible with this technology; and reinforcement of previously diagnosed clinical conditions can be brought back into our patients’ focus.
Implementing the latest intraoral camera technology into the dental practice clinical protocol can also give value-added factors to “wow” patients, prevent buyer’s remorse, and can also be used to boost reputation in today’s social media markets.
References
- Caufield PW. Dental caries: an infectious and transmissible disease. Where have we been and where are we going? N Y State Dent J. 2005;71:23-27.
- Van Winkelhoff AJ, Boutaga K. Transmission of periodontal bacteria and models of infection. J Clin Periodontol. 2005;32(suppl 6):16-27.
- Southward K. The systemic theory of dental caries. Gen Dent. 2011;59:367-375.
- Ramamoorthy RD, Nallasamy V, Reddy R, et al. A review of C-reactive protein: a diagnostic indicator in periodontal medicine. J Pharm Bioallied Sci. 2012;4(suppl 2):S422-S426.
- Nakano K, Nemoto H, Nomura R, et al. Detection of oral bacteria in cardiovascular specimens. Oral Microbiol Immunol. 2009;24:64-68.
- Abranches J, Miller JH, Martinez AR, et al. The collagen-binding protein Cnm is required for Streptococcus mutans adherence to and intracellular invasion of human coronary artery endothelial cells. Infect Immun. 2011;79:2277-2284.
- Bagramian RA, Garcia-Godoy F, Volpe AR. The global increase in dental caries. A pending public health crisis. Am J Dent. 2009;22:3-8.
- Papapanou PN. The prevalence of periodontitis in the US: forget what you were told. J Dent Res. 2012;91:907-908.
- Pickard M. Power to the people. Think Quarterly. September 2011. google.com/think/articles/power-to-the-people.html. Accessed November 12, 2013.
- Terrer E, Koubi S, Dionne A, et al. A new concept in restorative dentistry: light-induced fluorescence evaluator for diagnosis and treatment. Part 1: Diagnosis and treatment of initial occlusal caries. J Contemp Dent Pract. 2009;10:E086-E094.
- Rosenberg JM, Shuman L, Morgan A. Technology enhances caries diagnosis and treatment. Dent Today. 2011;30:162-166.
Dr. Rosenberg maintains a private practice in Philadelphia, Pa, emphasizing restorative and esthetic dentistry. He is a fellow of the AGD and holds associations with various restorative, esthetic, and orthodontic organizations. He publishes in this field to increase awareness of high-tech materials and procedures and performing dentistry more efficiently and with higher quality. Dr. Rosenberg places hundreds of bonded restorations monthly and has a patent pending in the area of nonmetal dental restorations. He is also the head of The Dental Healthcare Group, which provides high-quality continuing education in the Philadelphia area. He can be reached at (215) 592-4747 or via e-mail at [email protected].
Disclosure: Dr. Rosenberg discloses that the SoproLIFE camera was provided by ACTEON North America.
Ms. Papanier is a registered dental hygienist with The Dental Healthcare Group located in Philadelphia, Pa. Practicing dental hygiene since 1987, she is licensed to administer local anesthesia and strongly prefers treating patients who are periodontally involved. She strives to develop a professional and personal rapport with every patient she meets/treats as this has shown to be the best method of successful treatment and compliance between herself and her patients. She participates in many continuing education courses in order to stay on the cutting edge. She can be reached at [email protected].
Disclosure: Ms. Papanier discloses that the SoproLIFE camera was provided by ACTEON North America.
Ms. Abdullah is a registered dental hygienist (RDH) with the Dental Healthcare Group in Philadelphia, Pa, and has more than 30 years of experience in the field. She earned her degree at the Community College of Philadelphia in 1984. Prior to obtaining her RDH degree, Ms. Abdullah was a clinical dental assistant. She is licensed in local anesthesia and participates in numerous educational courses to advance her clinical skills, including soft-tissue management (phases 1 and 2), scaling and root planing, and utilizing ultrasonic instruments. She is also certified as a myofunctional therapist. She also has extensive training in Botox and Juvederm therapy. She has participated in various dental trials for companies such as Proctor and Gamble/Warner Lambert as well. She can be reached via e-mail at the address [email protected].
Disclosure: Ms. Abdullah discloses that the SoproLIFE camera was provided by ACTEON North America.


