


INTRODUCTION
Cosmetic dentistry is being sought out in record numbers, with experts saying the current market size of $29 billion could grow to nearly $60 billion before the end of the decade.1 Prospective cosmetic patients are coming into my office younger and younger, fueled by social media and near-constant comparison to Hollywood smiles.2
When considering restorative solutions for younger patients, clinicians must foremost be mindful of the long-term dental health of these patients. It’s imperative to consider the psychological effects of our treatment—or decision not to treat.2 Feeling self-conscious about one’s appearance—especially during crucial stages of development—can influence psychological well-being.
CASE REPORT
Featured in this case is a 15-year-old girl who presented near the end of her orthodontic treatment. Along with her mother, she came to me looking for an immediate solution to her “smile issue.”
As seen in her initial photographs (Figure 1), when we asked her for a big smile, she gave us a closed-lip smile. She’d trained herself to only smile with her lips closed.

Figure 1. When asked to smile, this young patient would only give a lips- pursed smile.
After a bit of coaxing, she gave us the smile in Figure 2. Her smile was very embarrassing for her. She had tooth size discrepancy, resulting in small teeth with gaps between them. Her mother explained she “wanted to have a smile like her friends.” The young woman’s lack of confidence in her smile was affecting her performance as a competitive cheerleader and made her feel inferior to her peers.

Figure 2. When coaxed, she finally revealed her teeth in a strained, open-lipped smile.
Patients such as this will often hear they’re too young for “permanent” treatment; they will have to wait until they reach 18 or 21 years of age, if not older, to receive their desired treatment.
With a very conservative approach to removing tooth structure, we can—and should—treat these patients. Their confidence and personality development relies on it.

Figure 3. Retracted view of dentition. Note engagers from clear aligner therapy were still in place.
Figure 3 shows the patient’s smile evaluation, displaying:
- The short lower one-third of her face
- Midline correct and occlusion, Class I
- Very small teeth with very little showing
- Multiple diastemas in the upper and lower teeth
- Dark shade
The goal was to have a more “toothy” smile—close all the spacing and improve the color while keeping the patient’s natural tooth structure.
Various treatment modalities were considered.
- Delay any treatment until the patient has reached maturity. As stated above, I believe waiting to address appearance issues such as this are detrimental to the patient.
- Direct composite bonding to close the spaces. If these spaces were simply closed with direct composite bonding, the proportion of the teeth would be wrong, and we would end up with a different aesthetic problem: short, fat teeth. Attempting to add length by cantilevering direct composite would not likely be successful in the long term.
- Indirect ceramic veneers of the maxillary teeth to close the spaces and add length. Gingival sculpting prior to veneer placement could add 1 to 2 mm of height to the teeth as well. Whitening of all other teeth would be included, as well as direct composite bonding to close the lower diastema.
Treatment 3 was ultimately selected.
Gingival sculpting was done to lengthen the teeth 1 to 2 mm. The Gemini Laser (Ultradent Products) was used. Figure 4 shows the right side sculpted with the left side not yet completed. Already, the teeth appear more appropriately sized.
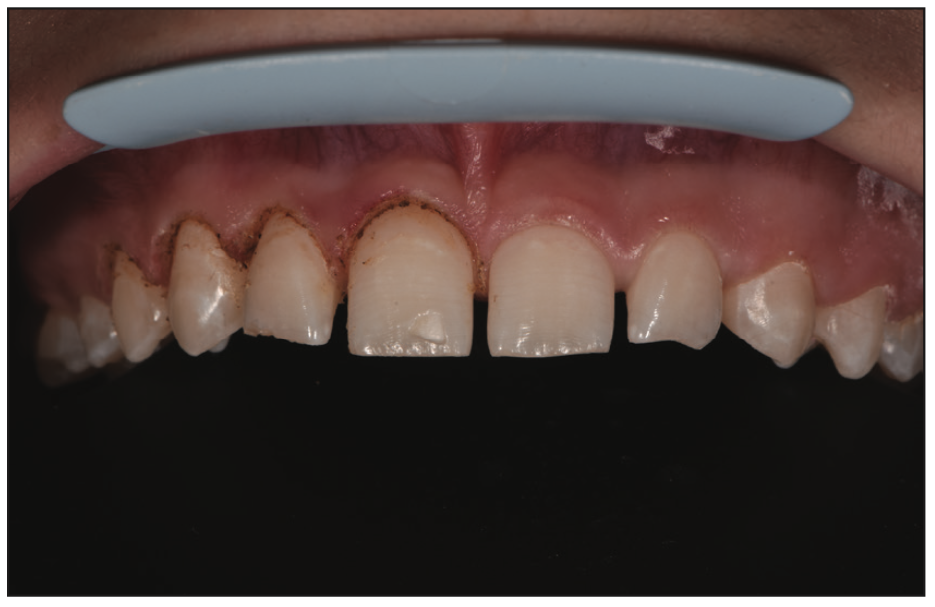
Figure 4. Gingival sculpting completed on the right side. The left side shows pre-sculpting gingiva architecture.

Figure 5. Minimal preparation of the teeth was done with sharp edges and corners being rounded for idealized ceramic adaptation.
Preparation for the ceramics was ultraconservative. Figure 5 shows the sharp corners were rounded and smoothed with discs—no further enamel was removed. The case was impressed, and provisionals were made.
The provisionals are the prototype for the final restorations, allowing a preview for the patient and clinician. In Figure 6, you’ll see occlusion and aesthetics were given a trial run. The patient wears the provisionals for a week or so, then returns to the office for evaluation.

Figure 6. Provisional restoration prototype.
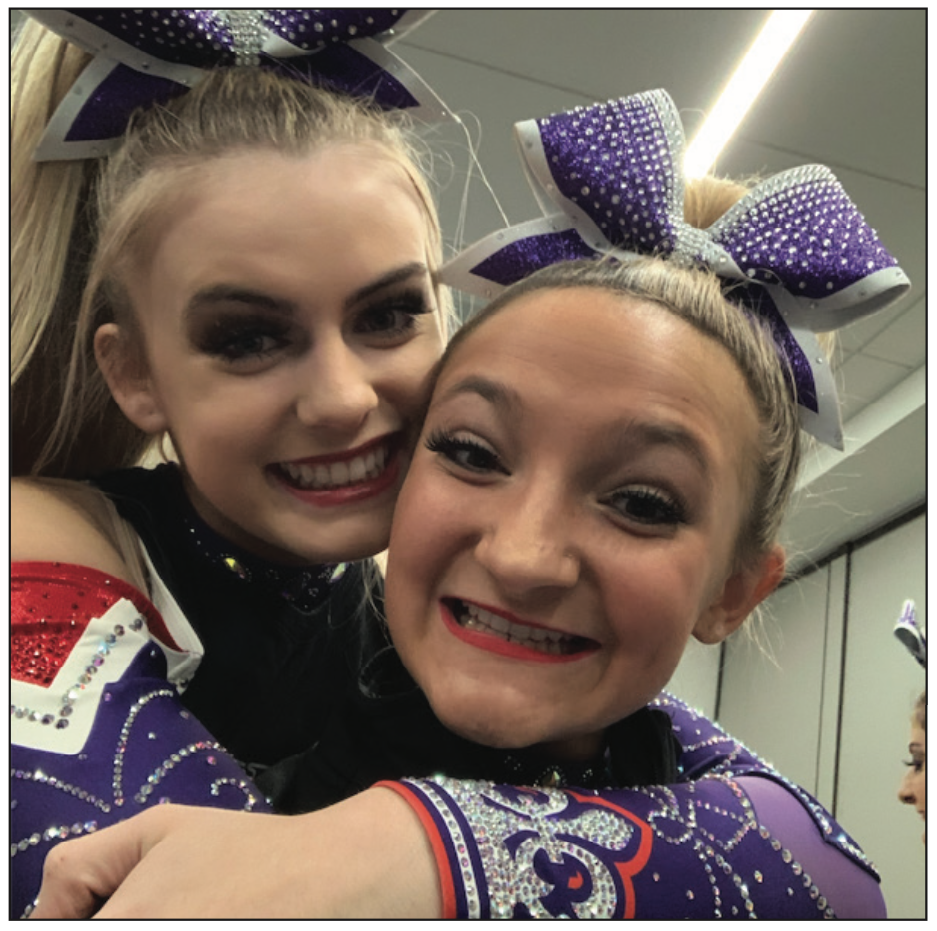
Figure 7. This photo was taken the day after the provi- sional prototype was placed. The joy and confidence the patient felt from her new smile was evident.
The day after prepping and placing the provisionals, our office received a text from the patient’s mother. The young woman was at a big cheerleading competition, and her mom took the photo in Figure 7. The text read, “Thank you, thank you, thank you!!! This is the first time I’ve seen her smile while she is cheerleading.”

Figure 8. Final restorations, adding length, improved shade, and smile “presence” (layered IPS e.max CAD restorations [Ivoclar] [Charles Moreno, Excel Studios]).

Figure 9. No more coaxing was necessary for this patient to smile. She radiates happiness with her smile now.
The veneers (layered IPS e.max CAD [Ivoclar]) were fabricated and placed. Her lower teeth were whitened using Opalescence Boost (Ultradent Products). The diastema between her lower central incisors was closed with direct composite bonding (Mosaic [Ultradent Products]) (Figure 8). Ceramics by Charles Moreno (Excel Studios) (Figure 9) completes the postoperative smile.
CONCLUSION
Self-image is part of the foundation of a developing sense of self-worth and self-esteem. Young adults with a positive self-image can grow with greater confidence, resilience, and independence, which can help them navigate challenges and setbacks throughout life.
As dentists, we have the opportunity to help these patients’ psychological well-being while doing so in a way that also promotes the long-term well-being of their oral health.
REFERENCES
1. Market Research Reports Service. Global cosmetic dentistry market size, share and COVID-19 impact analysis, by product type (dental systems and equipment, dental implants, dental implants, dental bridges, dental veneers, dental crowns, orthodontic braces and inalys & onlays), by end user (dental hospitals and clincs, dental laboratories and others), by age group (children and adults) and regional forecasts, 2022-2028. Markets N Research. 2022.
2. McMahon S. Selfie culture, young adults, and cosmetic dentistry: snapchat dysmorphia creates new aesthetic demands from teenagers and young adults. Dent Today. 2021;40(4): 52-57.
ABOUT THE AUTHOR
Dr. McMahon is a graduate of the University of Pittsburgh (Pitt) School of Dental Medicine. She maintains a private practice focused on cosmetic dentistry in Pittsburgh. Dr. McMahon is accredited by the American Academy of Cosmetic Dentistry (AACD) and is an invited Fellow of the prestigious American Society for Dental Aesthetics. She is a past clinical instructor in prosthodontics and operative dentistry at Pitt. Dr. McMahon frequently lectures across the United States on minimally invasive dentistry and conservative cosmetic dentistry for teenagers and young adults and has been annually voted by her peers as a top dentist in Pittsburgh for more than 20 years. She can be reached via email at drsusan@wowinsmile.com.
Disclosure: Dr. McMahon received an honorarium from Ultradent Products for writing this article.








