
Plastic has become a major driver in the multi-billion-dollar orthodontic industry. In fact, over the past few years, the advances in clear aligner technology have changed the landscape of the orthodontic practice modality.
In 2016, clear aligner technology garnered $1.1 billion in revenue, with $600 million produced in the United States and $400 million earned by orthodontists based in the United States.
As advances in clear aligner technology continue to soar, so does patient growth. In 2018, the number of patients with Invisalign rose by 24.2% in North America and 45% internationally. Likewise, 1.2 million new cases were started in 2018, garnering a record-breaking $2 billion in revenue.
Some literature argues that clear aligner treatment can create an anti-aging effect by boosting facial aesthetics and beauty. Clear aligner treatment also is less time-consuming than metal brackets and more ideal for adult patients with busy work schedules. Clear aligners require fewer office visits, significantly fewer dietary and hygienic restrictions, and fewer emergency visits. At-home maintenance is easier as well.
Additionally, the clear aligner appliance’s stability and retention can be beneficial for adult patients who have undergone extensive restorative treatment. Moreover, patients show a reduction in enamel demineralization compared to fixed treatments.
On the other hand, some studies argue that fixed appliances may be more effective in treating malocclusion, controlling teeth torque and rotations, and increasing transverse width and retention.
But when assessing adult patients’ compatibility with available orthodontic appliances like traditional braces and lingual braces, clear aligners show the most favorable results and the least amount of oral health problems, general activity disturbances, oral dysfunction, and eating disturbances. In conclusion, clear aligners are simple, they provide optimal results, and they are the most aesthetically pleasing option for adult patients seeking orthodontics.
Case Study 1: Class II, Division I Deep Overbite
A 32-year-old patient visited the practice stating that she did not like her overbite as well as several misaligned teeth in her upper and lower dental arches (Figure 1). Diagnostic records revealed a Class II, Division I malocclusion, severe 100% overbite, moderately excessive overjet, and mild upper and lower crowding (Figure 2).
Invisalign clear aligner therapy was the appliance of choice in treating the ma
 |
 |
| Figure 1: The 32-year-old patient did not like her overbite as well as several misaligned teeth in her upper and lower dental arches | Figure 2: Diagnostic records revealed a Class II, Division I malocclusion, severe 100% overbite, moderately excessive overjet, and mild upper and lower crowding |
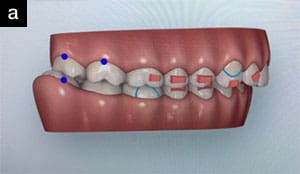
locclusion, and we used Invisalign’s ClinCheck software to digitally set up tooth movement (Figure 3). Treatment mechanics included upper anterior teeth intrusion, conventional bite ramps on the upper canines for deep bite mechanics, leveling the lower arch with reverse curve of spee built into the tooth movement setup, and Class II mechanics using Class II elastics from the upper canines to the lower first molars.
The patient was given a set of 12 clear aligners each appointment, with instructions to change the aligners every week. Appointments were scheduled every 12 weeks. A total of 36 active aligners accomplished deep bite and excessive overjet correction.
 |
 |
 |
| Figure 3: We used Invisalign’s ClinCheck software to digitally set up tooth movement |
 |
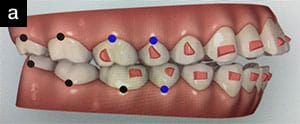
| Figure 4: In less than 12 months of treatment, the deep overbite was corrected, and the patient was ready for a refinement as the final stage of treatment. |
In less than 12 months of treatment, the deep overbite was corrected, and the patient was ready for a refinement as the final stage of treatment. There were only four active visits to the office, including taking the scan and removing attachments for refinement, emphasizing the efficiency of clear aligner therapy (Figure 4).
Case Study 2: Class II, Anterior Open Bite
A 22-year-old patient visited the practice with a chief complaint about her open bite (Figure 5). Diagnostic records showed a Class II subdivision left malocclusion, mild upper spacing, and a 5-mm anterior open bite, extending posteriorly to the second bicuspids (Figure 6).
 |
| Figure 5: The 22-year-old patient’s chief complaint was her open bite. |
 |
 |
| Figure 6: Diagnostic records showed a Class II subdivision left malocclusion, mild upper spacing, and a 5-mm anterior open bite, extending posteriorly to the second bicuspids |
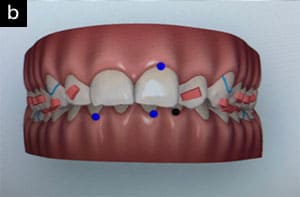
Again, we used Invisalign clear aligners to correct the patient’s malocclusion. The ClinCheck digital setup included a combination of posterior intrusion and anterior extrusion mechanics to close the anterior open bite (Figure 7). We suggested extracting the upper and lower third molars to help with posterior intrusion mechanics, but the patient decided not to proceed with extractions, and her open bite was successfully closed.
 |
 |
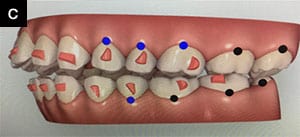 |
| Figure 7: The ClinCheck digital setup included a combination of posterior intrusion and anterior extrusion mechanics to close the anterior open bite. |
 |
 |
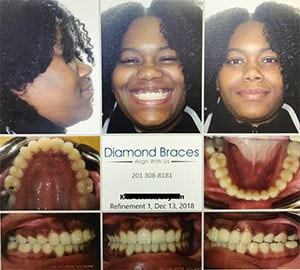
| Figure 8: The entire treatment time to close the anterior open bite and upper spaces was nine months. | Figure 9: Over the course of nine months of treatment, the patient only visited the practice five times, including appointments for the scan and refinement scan. |
The patient was given a set of 12 aligners every appointment with instructions to change aligners every week. Appointments were scheduled every 12 weeks. A total of 36 active aligners were used to correct the patient’s anterior open bite, close her upper spaces, and retract her upper anterior teeth.
The entire treatment time to close the anterior open bite and upper spaces was nine months (Figure 8). Further refinement was then planned for the finishing stage. Over the course of nine months of treatment, the patient only visited the practice five times, including appointments for the scan and refinement scan (Figure 9).
Dr. Rabinovich is an orthodontist at Diamond Braces. He earned his Doctor of Dental Medicine degree from the Rutgers School of Dental Medicine. He then traveled to Denver, Colorado, for specialty training in orthodontics and dentofacial orthopedics as well as to earn a master of science degree in dentistry at the University of Colorado-Anschutz Medical Campus. He is an active member of the ADA, the New Jersey Dental Association, and the American Association of Orthodontists (AAO). While in residency, he represented the Rocky Mountain Society of Orthodontists on the AAO Council on New and Younger Members.
Related Articles
CVS to Open SmileDirectClub Clear Aligner Shops in Its Pharmacies
Managing the Rising Trend of Adult Orthodontic Patients
More Adults Seeking Orthodontic Treatment

