
INTRODUCTION
In the July 2019 issue of Dentistry Today, we explored how modern implant design and simplified drilling protocols are making implant dentistry easier for the clinician, with improved patient outcomes. We will now explore recent innovations in extraction and immediate placement clinical protocols, and how they relate to modern implant engineering and design. Research related to implant engineering has been compiled through an expanding US implant manufacturing facility. Research related to the clinical efficiency procedures was done with cooperation from multiple DDSOs (dentist-owned DSOs) around the country. The goal of this article is to expand the reader’s clinical horizons and to dispel myths surrounding implant dentistry. Additionally, the information presented herein will demonstrate more options as they relate to the extraction and immediate placement combination.
 |
| Immediate Placement Infographic: iHex 1, iHex 2, MorsTorq, and iH Active (IH Biomedical) offer products that have ideal implant bodies, threads, and vent designs for immediate placement. |
Mastering Minimally Invasive Extraction Techniques
In the days before implant dentistry, it did not matter how much bone was left after an extraction. Many may remember times in dental school when professors removed vast amounts of buccal bone in the name of efficiency. Those days are gone, as the goal is now to maintain maximal bone with minimal trauma to surrounding tissues to benefit a potential implant site. As a profession, we are still in the early phase of the move to minimally invasive extractions, and the field is highly fragmented. The goal of this article is to cover some of the more popular and effective techniques currently used by implant enthusiasts. In a 2018 JADA article,1 vertical forces were examined as the primary forces used to extract a tooth. As the abstract noted, “Minimally invasive vertical tooth extraction techniques have evolved in light of the limitations of conventional tooth extraction techniques and flap surgery in preserving the alveolar bone. The authors conducted a study to obtain data on the performance of a vertical extraction system. This included comparing the need for flap surgery using the vertical extraction system vs conventional tooth extraction techniques for the extraction of anterior teeth and premolars not suitable for forceps extraction.” In conclusion, “the results suggest that the vertical extraction system may be used with a high success rate for extraction of severely destroyed teeth, and its use may lead to a marked reduction in the need for flap surgery. Randomized clinical trials are needed to confirm the findings.” This article showed that vertical forces, combined with several of the other techniques to be overviewed here, enhance bone retention and facilitate implant placement.
Most minimally invasive techniques rely on the exertion of forces (trauma) to the periodontal ligament of the tooth. This, in turn, creates hyaluronic acid buildup in the periodontal ligament space. The acid simultaneously breaks down the ligament and allows for a hydraulic pressure release in the socket. A combination of rotational, vertical, and light horizontal forces may then be used to atraumatically extract the tooth.
Dr. Brady Frank began offering mobile implant dentistry in more than 15 locations in the Pacific Northwest in 2008. On some days, he did well over 100 extractions and more than 30 implant placements with one surgical assistant. A good percentage of these cases were both removable and fixed full-arch cases, requiring efficient techniques, both in relation to the extraction technique and implant placement.
Let’s look at 3 favorite techniques adopted by clinicians around the country who have sought to understand the mechanics of atraumatic extractions.
 |
 |
| Figure 1a. Tooth No. 12 with deep distal caries necessitating extraction. Atraumatic extraction techniques were used to do the extraction, including rotational forces. | Figure 1b. The implant was placed immediately after thoroughly curvetting the socket site (MorsTorq [iH Biomedical]). |
1. The “Button Sewing” Technique
This technique utilizes a long-shaft, small round bur in your standard, slow-speed handpiece or implant handpiece. Some call it a “sewing” technique. Basically, the round bur is used to poke holes around the tooth while sliding down the root surface all around the tooth about 4.0 to 5.0 mm in depth (this area has the highest density of PDL fibers). This disrupts the PDL space, reduces hydraulic pressure, increases hyaluronic acid buildup, and allows for an estimated 40% to 50% reduction in extraction trauma. These benefits are based upon Dr. Frank’s experiences serving as a mobile extraction and implant provider.
2. The “Wiggle and Wait” Technique
This technique also leverages the buildup of hyaluronic acid because the tooth is placed under continuous force through forceps and/or elevation for 2 minutes. The clinician then leaves to do a hygiene exam or perform another brief check for a minimum of 10 minutes. By the time the extraction is re-engaged, the PDL is significantly weakened by the acid, and the extraction is thus easier and less atraumatic to the surrounding tissues.
3. The Modified Elevator Technique
This technique is very similar to the “wiggle and wait” technique. However, the instrument (elevator or luxator) is left in place as the clinician vacates the room for a minimum of 10 minutes. The instrument places continuous pressure on the periodontal ligament, generating hyaluronic acid buildup and loosening the ligament, which together provide the prerequisite for an efficient and atraumatic series of extractions. It is helpful to have several sizes of elevators available to achieve this technique. With full-mouth extraction cases, this technique can be initiated in one quadrant as another quadrant is being worked on.
 |
 |
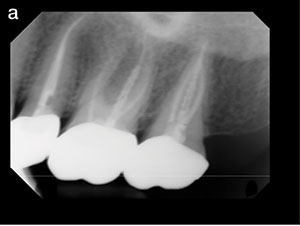
| Figure 2a. Tooth No. 14 with failing endodontic treatment requiring extraction. |
Figure 2b. The tooth was atraumatically extracted, utilizing techniques discussed in this ar ticle. A lance drill was used to drill down the center of the septal area. |
 |
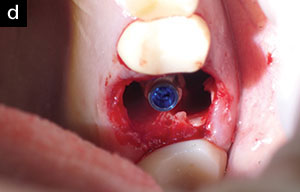 |
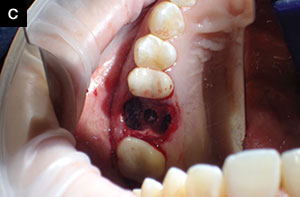
| Figure 2c. The final osteotomy was created in preparation for implant placement. | Figure 2d. The implant was inserted to a high degree of primary stability, about 3.0 mm below the external crest of the bone (MorsTorq). |
 |
 |
| Figure 2e. Grafting material was placed around the implant, with care taken to fill each of the 3 sockets individually. | Figure 2f. The area was sutured utilizing PRF. |
 |
 |
| Figure 2g. A radiograph after grafting material was placed and the area was sutured. | Figure 2h. The 6-week radiograph demonstrated good healing and solid bone response to the graft. |
Mastering Minimally Invasive Immediate Placement Techniques
Many clinicians do a lot of immediate implant placements when first starting to place implants. Historically, many seem to think the immediate implant procedure is less predictable with a higher failure rate than when implants are placed in fully or partially healed ridges. Statistically, this is true. Additionally, there are many more variables to consider when placing immediate implants vs delayed placement, including:
- angulation of the tooth
- crestal bone regression following the procedure
- placement of grafting material between the implant and socket wall
- achieving primary stability
- degranulating or delaminating socket walls
- socket wall defects
- presence of bacteria/apical radiolucency
- vertical periodontal defects
These issues tend to rear their ugly heads mid-procedure, which can throw schedules off and create undue stress. Even though experienced clinicians learn to solve many of these problems, unpredictability is still a significant variable. Therefore, many clinicians have chosen to extract, graft, and delay placement. Depending on the graft material, the implant may be placed in as few as 6 weeks or so, as opposed to months, making delayed placement seem all the more reasonable. Picking and choosing immediate placement cases based on a thorough inventory and reflection on the above variables ends up being the most prudent pathway. Taking time to reflect on these variables also helps prevent a lot of failures or less-than-desirable patient outcomes.
For clinicians who have gone through the learning curve and educated themselves, however, there are many advantages to immediate placement or delayed placement. A 2016 article in the European Journal of Oral Implantology sought to bring conclusive answers to the elusive question of whether to place immediately or to extract and wait for site healing.2 The authors’ purpose was to “compare the clinical outcome of single implants placed immediately after tooth extraction with implants placed 6 weeks after tooth extraction (immediate-delayed placement), and with implants placed after 4 months of extraction and socket healing (delayed placement).” Much to the pleasure of those who enjoy the placement of immediate implants, the following was concluded:
“No statistically significant differences for failures, complications, and patient satisfaction were observed when placing single implants immediately, 6 weeks or 4 months after tooth extraction; nevertheless failures and complications were more frequent for immediate and immediate-delayed placed implants. Bone level changes were similar between the different procedures, but the aesthetics showed better results for immediate and immediate-delayed implants.”
 |
 |
 |
| Figure 3a. Unrestorable tooth No. 10, requiring atraumatic extraction as the patient elected to have an immediate implant placement procedure. Rotational forces were used during the extraction to avoid damage to the facial plate of bone. | Figure 3b. A lance drill was used to redirect the implant path of insertion slightly to the mesial. |
Figure 3c. The final implant was placed with greater than 35 Ncm torque and proper anticipated positioning (MorsTorq). |
Extraction and Immediate Placement in Relation to Implant Engineering
Recent engineering technology breakthroughs have allowed for more efficient and predictable immediate placement. More aggressive and sharper threading, with more taper in the apical third of the implant, are innovations included in modern implant designs over the last couple of years. The immediate placement infographic (page 48) highlights the clinical advantages to modern engineering variations in implant dentistry. Likewise, the case examples (Figures 1 to 3) demonstrate the variety of cases with improved clinical ease directly due to those engineering innovations.
Often, the clinician is faced with a choice between options: to immediately place the implant in the anterior region or delay both placement and restoration. A recent article in Clinical Oral Implants reviewed immediate vs delayed placement in the anterior region.3 The study found the following to be the case:
“…timing of restoration seemed to positively affect the aesthetic outcomes of immediately placed implants as evidenced by higher median PES values for the immediate restoration group when compared to the delayed restoration group….It is therefore advantageous to place implants immediately following extraction in the anterior zone. Enhanced aesthetic outcomes appear to be due to preservation of the papilla height associated with the immediately placed implant and restoration.”
As far as success rates go, a 2015 article in the European Journal of Oral Implantology gives us a great overview to guide our clinical decisions.4 The purpose of the article is to “compare the effectiveness of immediate post-extractive single implants with delayed implants placed in preserved sockets after 4 months of healing. Implants that achieved an insertion torque of at least 35 Ncm were immediately non-occ
lusally loaded.”
The question is whether there is a higher failure rate with immediate implants receiving a non-occlusally loaded temporary. The good news is that the research has found that both procedures performed equally well:
“No significant differences were observed between the 2 procedures, although the only 2 implant failures were for immediate post-extractive implants. It seems more difficult to obtain an implant insertion torque superior to 35 Ncm in sockets preserved with algae-derived bone substitute after a 4-month healing period than at immediate post-extractive sites.”
The 2 implant failures examined in the study were both immediately placed. In order to ensure the highest success rate, there are several key tenets to follow from the research. In general, in soft- to moderate-bone density, it is best to under-prepare the osteotomy site to achieve high torque/primary stability. Make sure to anticipate minor bone resorption by placing the implant 1.5 mm subcrestal to the facial plate. Place grafting material between the socket wall and implant if the space is greater than 2.0 mm. Use an anterior stock abutment or temporary abutment to create a temporary crown, ensuring the elimination of any occlusal forces while checking all excursive movements. In cases where primary stability is unable to be achieved with a torque value greater than 35 Ncm, the prudent clinician should plan a 2-stage surgical procedure.
CLOSING COMMENTS
It is our hope that the case examples shared here create a greater understanding of the variables influencing atraumatic and efficient extractions and immediate implant placement. A thorough grasp of the subject matter creates confidence in providing these procedures, greater success, and improved patient outcomes.
Stay tuned for the next article in this series, as we explore more efficient and minimally invasive surgical techniques to add to your implant arsenal.
References
- Hong B, Bulsara Y, Gorecki P, et al. Minimally invasive vertical versus conventional tooth extraction: an interrupted time series study. J Am Dent Assoc. 2018;149:688-695.
- Felice P, Zucchelli G, Cannizzaro G, et al. Immediate, immediate-delayed (6 weeks), and delayed (4 months) post-extractive single implants: 4-month post-loading data from a randomized controlled trial. Eur J Oral Implantol. 2016;9:233-247.
- Arora H, Ivanovski S. Clinical and aesthetic outcomes of immediately placed single-tooth implants with immediate vs delayed restoration in the anterior maxilla: a retrospective cohort study. Clin Oral Implants Res. 2018;29:346-352.
- Felice P, Pistilli R, Barausse C, et al. Immediate non-occlusal loading of immediate post-extractive vs delayed placement of single implants in preserved sockets of the anterior maxilla: 1-year post-loading outcome of a randomized controlled trial. Eur J Oral Implantol. 2015;8:361-372.
Dr. Bessonet earned his DDS degree from the Louisiana State Univeristy School of Dentistry in 2003. He is currently the chief faculty member of the Louisiana Implant Institute. Dr. Bessonet is a member of the ADA, the American Academy of Implant Dentistry (AAID), the American Dental Society of Anesthesiology, and the International Congress of Oral Implantologists (ICOI). He has also achieved Fellowship in the AGD. He can be reached at [email protected].
Dr. Williams received his DDS degree from the Texas A&M College of Dentistry. He is in private practice with his brother in Allen, Texas. He is an alumnus of the Las Vegas Institute for Advanced Dental Studies and is an associate Fellow of the American Academy of the AAID. He can be reached via email at [email protected].
Dr. Severson earned his DDS degree from the University of Minnesota School of Dentistry. He co-founded the Minnesota North Implant Institute and serves as chief faculty for the institute. He also serves as adjunct faculty of the Dallas Implant Institute. Dr. Severson is a member of the ADA and the Minnesota Dental Association and practices in Aitkin and Crosby, Minn. He can be reached via email at [email protected].
Dr. Frank is an international clinical and business lecturer, inventor and founder of multiple companies in the dental and real estate development space. Since graduating from Marquette University School of Dentistry in 2001 he has been the founder, and co-owner, in multiple private dentist-owned groups (DDSOs). He can be reached at [email protected] or DDSOlive.com.
Disclosures: The authors have a financial interest in some of the products mentioned in this article but received no compensation for writing it. All authors are paid faculty members for IH Biomedical.
Related Articles
Immediate Implantation in a Deficient Ridge: A Predictable Treatment Protocol
Aesthetic Success in the Anterior Region: Immediate Placement and Temporization

