
Written by: Dr. Munther Sulieman
A 45-year-old patient, who reported smoking approximately 15 cigarettes per day and consuming 10 units of alcohol per week, attended the clinic for the first time seeking emergency care. He had no significant medical history. His main complaint was a fractured lower left first molar (LL6; tooth No. 36), which had produced a sharp edge that was causing trauma to the lateral border of his tongue, resulting in ulceration and discomfort during eating.
The patient was not a regular at the clinic and typically seeks treatment only when experiencing acute problems. He requested an immediate solution and expressed no strong preference regarding the retention or extraction of the tooth, provided the issue was resolved in 1 visit.
Clinical examination revealed that LL6 contained a large, aged amalgam restoration, with fracture of the remaining mesio-lingual cusp. Due to the patient’s unwillingness to undergo multi-visit treatment, and the absence of an on-site milling facility, indirect restorative options were not feasible. This narrowed treatment to 2 practical options: placement of a direct buildup interim core restoration to remove the sharp edge, or extraction of the tooth to definitively eliminate the source of tongue irritation and allow mucosal healing.
In determining the best restorative approach, both the patient’s desire for the quickest possible treatment and the substantial size of the cavity were key factors. Given the clinic’s transition away from dental amalgam, a bulk-fill composite was a natural choice. Although most light-cured bulk-fill materials are recommended for placement in increments of up to 4 mm,¹ the depth of this cavity exceeded that limit, which would have necessitated multiple layers. As the patient strongly preferred to minimize time in the chair, a restorative material that reduced procedural steps was advantageous.
The options were therefore narrowed to Aura Bulk Fill (SDI), which the manufacturer states can be cured in 5-mm increments, or Stela (SDI), a self-cure bulk-fill composite requiring no light curing. Stela offered the most efficient workflow while meeting all clinical requirements for restoring the tooth in this context. Its self-curing properties avoided the need for incremental light curing, reducing chair time and providing a practical, patient-centered solution.
Clinical Procedure
Following clinical examination of the fractured tooth, a periapical radiograph was taken to assess for any atypical pathology (Figure 1). Sensibility testing was performed using ethyl chloride (EndoFrost [Roeko]) and an electric pulp tester (Digitest [Parkell]). Both tests elicited positive responses with no lingering sensation after removal of the stimulus. These findings indicated a vital pulp, eliminating the need for root canal treatment at this stage. This outcome aligned well with the patient’s preference to avoid multi-visit procedures, such as endodontic therapy, which would likely have led him to opt for extraction.

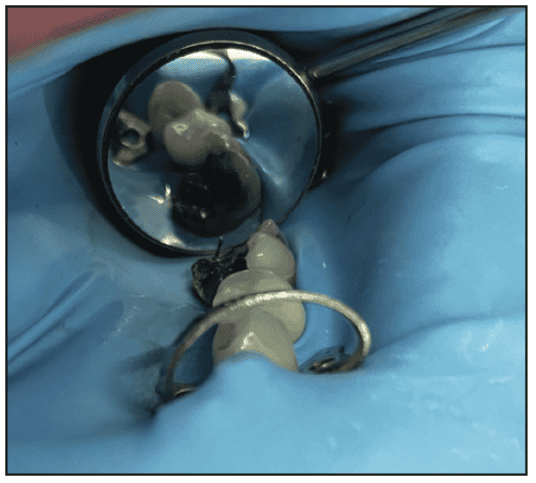
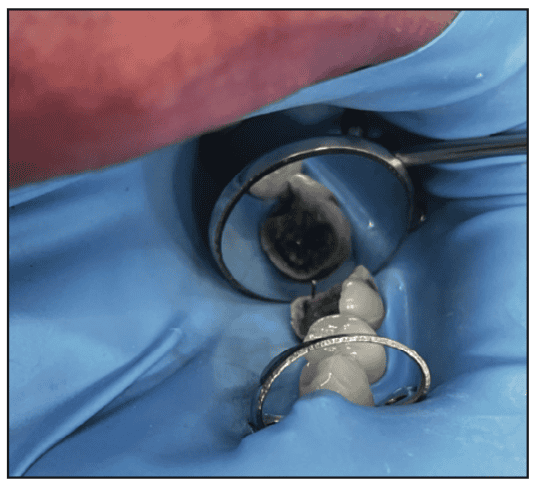
Local anesthetic was provided via an inferior alveolar nerve block, after which the tooth was isolated using a rubber dam (Figure 2). The old amalgam restoration was removed by sectioning it with a tungsten carbide bur in a high-speed handpiece, creating a cross-cut pattern to the full depth of the restoration. The fragmented amalgam pieces were then carefully lifted out using an excavator to minimize drilling and reduce the risk of further loss of tooth tissue (Figure 3).

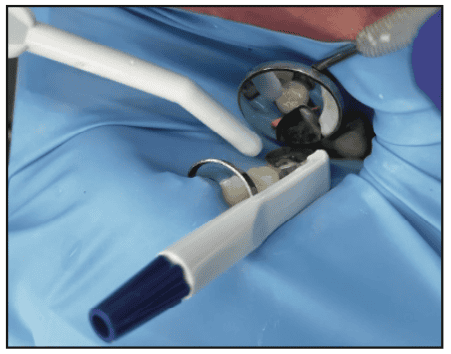
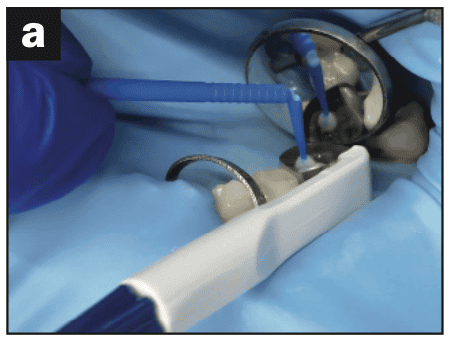
The resulting cavity was free of caries and was air-abraded to freshen the margins and remove residual amalgam corrosion products. This enhanced micromechanical retention and supported improved bonding of the composite to the tooth structure. Air abrasion also reduces the risk of the “white line” phenomenon at the cavity-restoration interface, which is associated with polymerization shrinkage inducing micro-fractures of unsupported enamel prisms and subsequent formation of marginal microgaps.² The cavity was then thoroughly rinsed and dried before placement of a wide Pro-Matrix Blue band (Young Innovations) and wedge (Figures 4 and 5). Stela primer was applied to all surfaces of the cavity using a microbrush, left in place for 5 seconds, and then air-dried for a further 2 to 3 seconds. Stela composite comes in 2 delivery systems—capsule and Automix syringe (Figure 6)—both based on UDMA (urethane dimethacrylate), GDMA (glycerol dimethacrylate), and 10-MDP (methacryloyloxydecyl dihydrogen phosphate), with slight variations in filler content that influence handling and final surface characteristics. For this case, the Automix syringe was selected. The syringe’s metal applicator tip was gently bent to provide optimal access to the base of the cavity. Its flexibility is advantageous when restoring deep or difficult-to-reach cavities in posterior teeth.

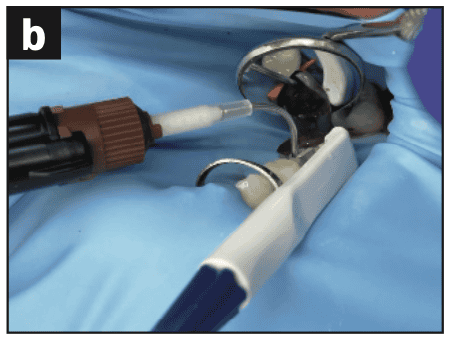
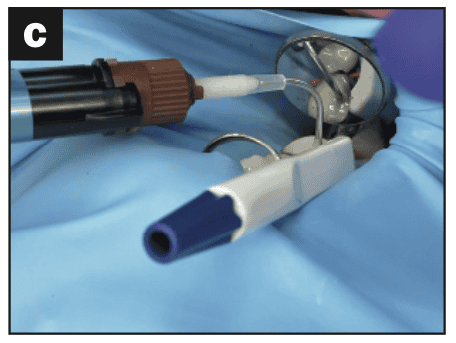
The cavity was restored in a single increment. The metal tip was positioned at the base of the cavity, and Stela composite was extruded slowly, withdrawing the tip as the composite level rose while keeping it submerged to prevent incorporation of air bubbles or voids. The progressive stages of the procedure are shown in Figure 7.
After placement, minimal sculpting was carried out before glycerine gel was applied to the surface to prevent formation of an oxygen-inhibited layer. A small amount of composite was dispensed onto the back of the clinician’s glove to monitor setting without disturbing the restoration. Initial trimming and polishing is typically feasible within 2 to 2.5 minutes from the start of composite placement.
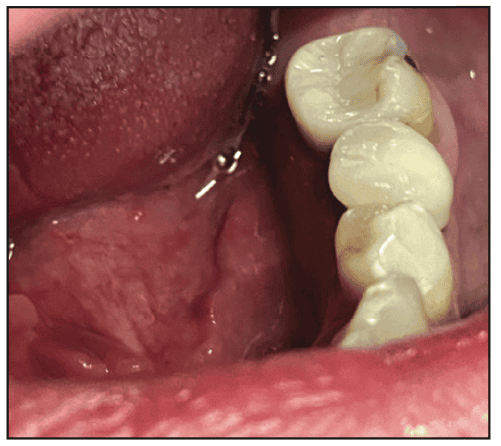
Once the composite had polymerized sufficiently, the matrix band and wedge were removed. The restoration was preliminarily trimmed using yellow-banded fine diamond burs. The rubber dam was removed, occlusion was checked, and diamond-impregnated polishing wheels were used to achieve the final finish. Within approximately 1 hour, Stela reaches around 90% of its full polymerization, significantly higher than the 40% to 45% conversion reported for most conventional light-cured composites. The final result (Figure 8) provided an efficient and satisfactory outcome, much to the patient’s delight.
The Stela primer, which contains methacrylates including 10-MDP, bonds chemically to enamel and dentine while also creating micromechanical retention via tags into dentinal tubules. As a contact primer, it polymerizes together with the Stela composite via a self-cure mechanism characterized by low polymerization stress. This results in polymerization beginning at the cavity margins and progressing in a controlled manner throughout the restoration, thereby reducing overall stress at the adhesive interface.³
Stela utilizes a rapid hydroperoxide-initiated, tertiary-amine free curing system. This initiates a fast “snap set” cure, during which monomers convert into polymer chains that rapidly crosslink to form a dense, interconnected network. This integrates both the fillers and the amorphous silica, resulting in a very resilient and strong composite material.
The 2 Stela delivery systems differ in filler composition and load, but both produce durable, long-lasting restorations. The capsule form contains a filler load of 77 wt% (55 vol%), comprising fluoro-alumino-silicate glass, ytterbium trifluoride, silicon dioxide, and calcium aluminate, with particle sizes ranging from 2 to 8 µm (median 4 µm). In contrast, the Automix syringe contains 61 wt% (36 vol%) filler, with an additional barium-alumino-borosilicate glass component and a narrower particle range of 2 to 5 µm (median 2.8 µm). These smaller fillers contribute to the more lustrous surface finish achieved with the Automix system, whereas the capsule system tends to produce a more matte appearance.3
The capsule delivers a firmer, more sculptable material, similar in feel to traditional packable composites, which some clinicians may favor for contouring after completing a single-increment fill. The Automix syringe, by contrast, produces a smoother, more flowable composite that typically requires finishing and refinement with diamond burs once initial polymerization occurs.
Although Stela is a relatively recent entrant to the dental market, developed as part of the global transition away from amalgam following the Minamata Convention (2013), its performance extends well beyond that of a simple amalgam alternative. After nearly 2 years of clinical use, it has become clear that Stela functions as an “all-rounder” in contemporary restorative dentistry, proving useful in a wide range of clinical scenarios. Its impressive mechanical properties and bioactive potential provide clinicians with confidence in its long-term reliability and efficacy in the oral environment.4-6
For more information call (800) 228-5166 or visit sdi.com.au.
REFERENCES
- Alrahlah A, Silikas N, Watts DC. Post-cure depth of cure of bulk fill dental resin-composites. Dent Mater 2014. Feb;30(2):149-154.
- Mandikos, Michael. “Better Composite Margins-Minimising the ‘ White Line .’” Australiasian Dental Practice Magazine 2007, July-August: 180–184.
- Price R. 2025 Thermal changes as Stela polymerises in a tooth when Stela primer is used. https://www.youtube.com/watch?v=HpV_O6XyD6k
- Alessandro D Loguercio et al. Clinical evaluation of a new chemically-cured bulk-fill composite in posterior restorations: 6-month multicentre double-blind randomized clinical trial. Journal of Dentistry, October 2024, Volume 149
- Dental Advisor Lab Tests: https://dentaladvisor.com/wp-content/uploads/2024/10/CE-Stela-SDI_web.pdf
- Laporte C et al. Mechanical, Antibacterial, and Physico-Chemical Properties of Three Different Polymer-Based Direct Restorative Materials: An In Vitro Study. Polymers 2025, 17, 1272

