
Written by: Drs. Kelly J. Blodgett, Varo Boyer, and Prof. Etyene Schnurr, and CDA Katie Mead
INTRODUCTION
Zirconia dental implants are increasingly recognized as viable alternatives to titanium implants, offering notable advantages in terms of biocompatibility, aesthetics, and patient preference for metal-free treatment. As demand for biologically favorable, aesthetically driven solutions increases, zirconia implants have gained clinical attention, particularly among patients with metal sensitivities or chronic systemic conditions.
This article synthesizes recent clinical evidence, including data from a practice-driven study in the United States, to provide a comprehensive overview of zirconia implant performance, survival rates, and strategies for successful clinical integration.
In November 2023, a clinical program was launched to assess the real world effectiveness of zirconia implants. This marked the beginning of a structured prospective clinical series designed to assess the real-world effectiveness of zirconia implants. The study assembled a team of experienced surgeons dedicated to incorporating zirconia implants into their daily practice, while contributing to research and education efforts.
This clinical study, named the Ceramic Implant Expert Team (CIET) project, was developed under a rigorously reviewed protocol approved by an Institutional Review Board and formally registered with ClinicalTrials.gov (Identifier: NCT06314425). This is the first registered clinical trial in the US to evaluate zirconia implants by practicing clinicians.
The primary objective of the CIET project was to assess the clinical efficacy of 1-piece, tissue-level zirconia implants supporting single crowns over a 12-month or longer follow-up period. The key outcome measures included the following:
- Cumulative Survival Rate (CSR)
- Gingival Profile
- Marginal Bone Level (MBL)
- Pink Esthetic Score (PES)
To ensure protocol consistency and clinical success, comprehensive training and on-site surgical support were provided to all participating centers. The active involvement of SDS ambassadors, experienced clinicians with extensive expertise in zirconia implantology, was instrumental in guiding the participants through the learning curve and maintaining adherence to the study protocol.
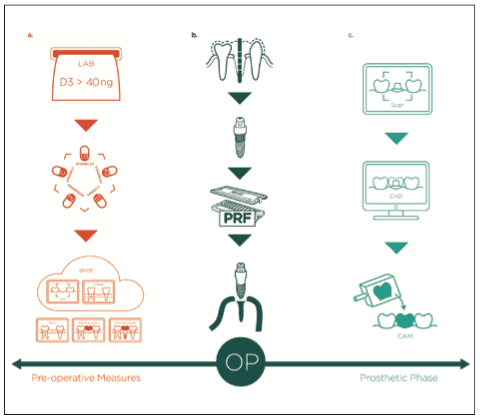
This article presents early clinical evidence from the CIET project, including followup outcomes and detailed documentation of 3 representative case studies. The cases are presented step by step, from surgical placement to prosthetic delivery, providing a clear framework that illustrates how zirconia implants can be effectively integrated into clinical workflows (Figure 1).
Case Series
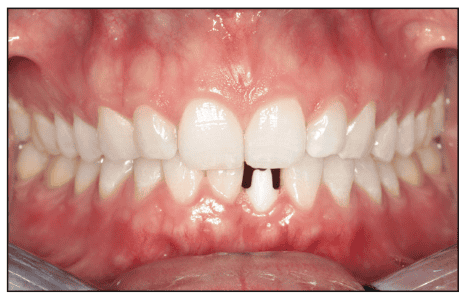
Data from 3 female patients (average age 47.16 years) who underwent immediate zirconia implant placement between August 2024 and October 2024, including radiographs and medical records, were prospectively analyzed. All implants were placed supracrestally in the maxilla (tooth Nos. 7 and 8) and the mandible (tooth No. 24). These patients required implant placement because of similar underlying issues: persistent periapical lesions in previously unsuccessful endodontically treated teeth, ill-fitting crowns, and periodontal deterioration. All participants provided informed consent for treatment and the use of anonymized data for publication. The patients were monitored for an average of 8.85 months following surgery, including a period of 4 months after implant placement. Radiographs and intraoral scans were obtained before and after implant placement, and follow-up images were captured and compared with those obtained after the final prosthetic restorations (Figures 2 to 4).

Treatment Plan
Following clinical examination, CBCT (Axeos [Dentsply Sirona]) was performed to assess the underlying bone and complete the diagnosis of the disease. All 3 patients met the CIET project’s inclusion criteria; therefore, 1-piece tissue-level zirconia implants were selected for placement.
According to the protocol, the treatment involved immediate implant placement, with a provisional crown cemented on the same day. A precise 3D virtual smile design based on aesthetic parameters and proportions (CEREC [Dentsply Sirona) was prepared by overlaying digital data and segmenting intraoral scanners (IOS) and CBCT data (SMOP [Swissmeda AG]). The integration of DICOM and STL segmentation into the planning software facilitated visualization of the tooth extraction, alveolar analysis, and optimization of surgical procedures. Digital implant planning was initiated in all cases (Figure 2a).
All 3 patients received supplementation due to plasma vitamin D3 levels below 40 ng/mL in the preoperative tests. The supplementation protocol suggested for these patients was based on previous studies and is outlined as follows: mineral and vitamin supplementation was prescribed for 4 weeks before and after surgery. Daily doses of magnesium, vitamins C, D3, K2/MK7, and Omega 3 were administered in simple-dose blister sachets (Big 5 [SDS Swiss Dental Solutions Inc]). Nutrabeads globules (approximately 2.5 mm in diameter) allowed for the controlled combined delivery of all supplements in a single, easy-to-swallow dose, promoting high patient adherence. This included a precise ratio of vitamin D to K2/MK7 (10,000 IU of vitamin D to 100µg of K2/MK7). Only patients with vitamin D levels of 40 ng/mL underwent surgery to ensure appropriate systemic conditions for bone healing after surgery.1,2 Pain was controlled with 1g of paracetamol, if needed.
Surgery Procedure
The implants were placed using a minimally invasive technique without vertically releasing incisions under local anesthesia (articaine 40 mg/mL with epinephrine 10 mg/mL [Sanofi]) and were uniform for all patients. The same surgeon placed the implants in all the patients. Rigorous inspection and curettage of surgical sites were performed. Advanced platelet-rich fibrin (A-PRF) produced using the Low-Speed Centrifugation Concept (Mectron Deutschland Vertriebs GmbH) was placed at the surgical site, over, and around the implant.3 Alveolar ridge augmentation and suturing were not required.
Provisional Crowns
All patients received a high-precision, passive-fit provisional crown cemented using GC Fuji Plus (GC America) straight glass ionomer cement on the day of surgery (Figure 2f and 3g). The implant shoulder of SDS implants can be safely reduced by up to 0.5 mm and angled to 30°. Using single-use, sterile, fine-grain diamond burs (46µm, red stripe) under continuous spray jet cooling (50mL/min), the crown margin was precisely adapted to the gingival contour. This technique ensures a natural emergence profile, while maintaining implant integrity and patient safety. When the provisional crowns were not predesigned and milled, the arches were scanned using a Primescan intraoral scanner (Dentsply Sirona), and provisional crowns were then designed and fabricated in-house using a CEREC machine (Dentsply Sirona). In both cases, this approach eliminates the need for additional abutments, appointments, and adjustments, thus reducing costs and treatment time (Figures 2d, 3, 4i, and 4k). The coronal design and tissue-level placement of SDS implants offered reliable soft tissue support, promoting healing and maintenance of keratinized gingiva, with reduced risk of recession (Figure 3).4,5 The occlusion was adapted to distribute occlusal forces evenly throughout the healing phase.
Definitive Crowns
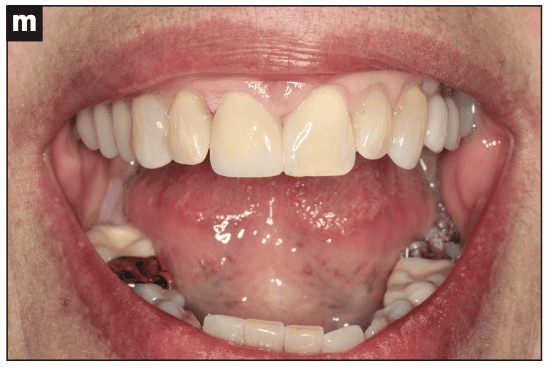
Final restorations were placed approximately 4 months after implant placement and healing. Temporary crowns were removed, and implant integration was confirmed using AnyCheck (NeoBiotech)6 in conjunction with a gingival contour assessment.7 Layered zirconia crowns were chosen for their superior aesthetics and color matching, making them ideal for anterior or highly visible regions, as in all 3 cases. Definitive crowns were cemented with glass ionomer cement (GC Fuji Plus), and occlusion was thoroughly evaluated (Figure 4m). Patients received oral hygiene instructions and a tailored maintenance plan. Patient satisfaction was high, with symptoms such as pressure, odor, and headaches resolved after zirconia implant rehabilitation. The result was both functional and aesthetically pleasing, completed in just 2 post-implant appointments.

Clinical Outcomes
All measurements were performed in accordance with the Ceramic Implant Rehabilitation Consensus Statements from the Joint Congress for Ceramic Implantology (2024) and followed the CIET project protocol. The cumulative implant survival rate was 100%, with all 3 implants remaining in place. Vertical bone loss was minimal and not statistically significant after 8.87 months (P = 0.1894). The difference in probing depth before and after placement of the definitive crown was 0.029 ± 0.12 mm (P = 0.8218), also not statistically significant.
No changes were observed in mobility (Class I, II, or III), plaque index, modified gingival index, or bleeding on probing compared to baseline. The change in keratinized gingiva showed a mean difference of 0.75 ± 0.80 mm (P = 0.3896). PES increased from 10.33 to 10.93 (P = 0.8676).
Data were analyzed using the mean and standard deviation. Statistical comparisons were performed using a 2-tailed paired t-test with a 95% confidence level, and P < 0.05.
DISCUSSION
Zirconia implants have shown high levels of success and survival in delayed and immediate implantation.8 We presented early results from the CIET project, which aimed to assess the clinical integration of zirconia implants in routine practice. The project emphasized structured training, ongoing mentorship, and hands-on surgical support for elements considered crucial to help practitioners overcome common challenges such as the learning curve and unfamiliarity with zirconia, especially for those transitioning from titanium implants.9 The clinical outcome measures collected also contribute to establishing a sustainable framework for future research and provide real-world, evidence-based insights from experienced clinicians who have adopted, or are considering adopting, zirconia implants into their workflows. The transition to zirconia implants also fosters ongoing professional development and aligns with the evolving, patient-centered demands of modern dentistry.10
From an economic standpoint, the use of 1-piece, tissue-level zirconia implants within an immediate loading protocol proved to be cost-effective, benefiting both clinicians and patients.9,11 Minimally invasive, backward-planned surgeries are well suited for zirconia implants, providing greater predictability with fewer required consultations, reduced stress, and enhanced safety. Zirconia’s inert properties, especially its resistance to corrosion and lower bacterial plaque adhesion compared with titanium, make it an ideal choice for metal-free dentistry, promoting soft tissue integration and minimizing the risk of peri-implant diseases.12-14
Favorable soft tissue responses and aesthetic outcomes further support the use of zirconia implants. These implants have demonstrated high mucosal compatibility, with low rates of inflammation and recession. In this study, the PES4, a widely accepted tool for evaluating aesthetic outcomes in implant dentistry, yielded positive results, as did the gingival profile.5 Mechanical performance and implant design also play a crucial role.15 Tissue-level zirconia implants are associated with high survival rates and fewer mechanical complications, largely due to the absence of a microgap between the implant and abutment.16 Recent advances in zirconia implant surface treatments have markedly improved both mechanical strength and osseointegration, addressing many of the limitations observed in earlier generations.
Particularly in the aesthetic area, the choice of a tissue-level system simplifies the surgical and restorative workflow, resulting in reduced chair time, lower costs, and less procedural stress.17
In addition to the clinical and mechanical benefits, biological integration and patient-reported outcomes further support the use of zirconia implants. Bone-to-implant contact for zirconia implants typically ranges between 67% and 73%, comparable to or even exceeding the values reported for titanium. These results are backed by both animal studies and human clinical trials.18 From the patient’s perspective, the aesthetic appeal and biocompatibility of zirconia contribute to high satisfaction, particularly among those seeking metal-free alternatives.10
Despite these advantages, zirconia implants pose specific challenges, especially for clinicians accustomed to titanium systems. A distinct learning curve exists, necessitating education, hands-on experience, and a willingness to adapt. However, the CIET project demonstrated that with proper guidance and a reliable system, zirconia implants can deliver highly predictable results, even in posterior regions and full-arch rehabilitation. Continued research- and practitioner-driven initiatives are expected to further improve their clinical performance and expand their applications in implant dentistry.
Acknowledgements
We would like to acknowledge Dr. Nicolas Elian for serving as the principal investigator of the CIET Study.
REFERENCES
1. Schnurr E, Volz KU, Mosetter K, et al. Interaction of telomere length and inflammatory biomarkers following zirconia implant placement: a case series. J Oral Implantol. 2023;49(5):524–31. doi:10.1563/aaid-joi-D-22-00236
2. Ghanaati S, Choukroun J, Volz KU, et al. One hundred years after vitamin D discovery: Is there clinical evidence for supplementation doses? Int J Growth Factors. 2020;3(3):3-11. doi:10.4103/GFSC.GFSC_4_20
3. Ghanaati S, Booms P, Orlowska A, et al. Advanced platelet-rich fibrin: a new concept for cell-based tissue engineering by means of inflammatory cells. J Oral Implantol. 2014;40(6):679–89. doi:10.1563/aaid-joi-D-14-00138
4. Schnurr E, Sperlich M, Sones A, et al. Ceramic implant rehabilitation: Consensus statements from Joint Congress for Ceramic Implantology: Consensus statements on ceramic implant. J Oral Implantol. 2024;50(4):435–45. doi:10.1563/aaid-joi-D-23-00083
5. Rutkowski R, Smeets R, Neuhöffer L, et al. Success and patient satisfaction of immediately loaded zirconia implants with fixed restorations one year after loading. BMC Oral Health. 2022;22(1):198. doi:10.1186/s12903-022-02231-0
6. Alkhouri S, Smeets R, Stolzer C, et al. Does placement of one-piece zirconia implants influence crestal bone loss? Retrospective evaluation 1 year after prosthetic loading. Int J Oral Implantol (Berl). 2023;16(1):43-51.
7. Monje A, Salvi GE. Diagnostic methods/parameters to monitor peri-implant conditions. Periodontol 2000. 2024;95(1):20-39. doi:10.1111/prd.12584
8. Mohseni P, Soufi A, Chrcanovic BR. Clinical outcomes of zirconia implants: a systematic review and meta-analysis. Clin Oral Investig. 2023;28(1):15. doi:10.1007/s00784-023-05401-8
9. Neugebauer J, Schoenbaum TR, Pi-Anfruns J, et al. Ceramic dental implants: a systematic review and meta-analysis. Int J Oral Maxillofac Implants. 2023;38(suppl):30–6. doi:10.11607/jomi.10500
10. Schnurr E, Parra M, Bauder R, et al. Patient perspectives on immediate zirconia implant therapy: results from a long-term multicenter European study. J Oral Implantol. 2025;51(5):444–53. doi:10.1563/aaid-joi-D-25-00111
11. Schnurr E, Schick F, Notter F, Lechner J, Schulz C, Volz KU. Oral health as a determinant in preventing cellular aging and promoting immune sustainability. J Clin Dent Oral Care. 2025;3(1):1–11.
12. Zhang C, Zhao X, Qiao S, et al. Peri-implant tissue alteration around tissue-level and bone-level implants in fresh extraction sockets: a histomorphometric study in dogs. Ann Transl Med. 2021;9(4):335. doi:10.21037/atm-20-8074
13. Schwarz F, Derks J, Monje A, et al. Peri-implantitis. J Periodontol. 2018;89 Suppl 1:S267–90. doi:10.1002/JPER.16-0350
14. Wang HL, Avila-Ortiz G, Monje A, et al. AO/AAP consensus on prevention and management of peri-implant diseases and conditions: Summary report. J Periodontol. 2025;96(6):519–41. doi:10.1002/JPER.25-0270
15. Pera F, Carossa M, Bagnasco F, et al. Comparison between bone-level and tissue-level implants in immediate-loading full-arch rehabilitations: a retrospective multi-center 1-year follow-up study. Prosthesis. 2023; 5(4):1301–11. doi:10.3390/prosthesis5040089
16. Schroeder HE, Listgarten MA. The gingival tissues: the architecture of periodontal protection. Periodontol 2000. 1997;13:91-120. doi:10.1111/j.1600-0757.1997.tb00097.x
17. Balmer M, Spies BC, Kohal RJ, et al. Zirconia implants restored with single crowns or fixed dental prostheses: 5-year results of a prospective cohort investigation. Clin Oral Implants Res. 2020;31(5):452–62. doi:10.1111/clr.13581
18. Balmer M, Payer M, Kohal RJ, et al. EAO Position Paper: Current level of evidence regarding zirconia implants in clinical trials. Int J Prosthodont. 2022;35(4):560–6. doi:10.11607/ijp.8131
ABOUT THE AUTHORS
Dr. Blodgett is a pioneer in the field of modern biological dentistry and holistic oral health. He is an author, researcher, international lecturer, and world-class clinician. His weekly social media posts,”Toxic Tuesday” and “Wellness Wednesday” have received international attention and acclaim as he educates and informs people throughout the world about the links between oral and systemic health. Through his book, Feel Whole Again – Your Humanistic Guide to Healthcare, and his clinical practice, he is introducing humankind to a synergistic, collaborative approach to health and wellness. He can be reached at [email protected].
Ms. Mead is a highly experienced dental assistant licensed in Washington and Oregon with more than 10 years of experience in general and biological dentistry. She holds EFDA, RDA, and CDA credentials and certifications in radiology, ACLS, phlebotomy/IV, and anesthesia with IV function. Among the first 50 Oregon EFDAs licensed in local anesthesia, she remains committed to learning and growing. Katie also holds a degree in Applied Science in Child and Family Studies with a certificate in Early Literacy. She can be reached at [email protected].
Dr. Boyer graduated from the UCLA School of Dentistry in 2008 and completed advanced GPR training at Cedars-Sinai and the VA. Since 2010, he has practiced in Los Angeles and joined the UCLA faculty in 2011. He trained in the UCLA Dental Implant Continuum and was the lead investigator in a global ceramic implant study. He is active in implant organizations and has recently joined the board of the International Academy of Ceramic Implantology. He teaches dental students, dental residents, and practicing dentists. He can be reached at [email protected].
Prof Schnurr is a Brazilian-born dentist and researcher based in Switzerland, specializing in ceramic implantology and the oral microbiome. She holds a PhD in Pharmacology and Medical Chemistry. Since 2022, she has served in clinical affairs and scientific studies for Swiss Dental Solutions, Switzerland. Her research explores the relationship between oral microbiota and systemic diseases, focusing on zirconia implants and on biological dentistry. She practices in Zurich and Kreuzlingen, contributing to both clinical care and scientific advancements in metal-free implantology and biocompatible treatment protocols. She can be reached at [email protected].
Disclosure: Dr. Blodgett is a KOL and US Ambassador for Swiss Dental Solutions. Prof. Dr. Schnurr is responsible for and is the study coordinator of the CIET study. The authors have received no compensation for writing this article.


