
Results of conventional whitening procedures have always been unpredictable, and in particular, successfully whitening tetracycline stained teeth and teeth with fluorosis has historically been nearly impossible. Few dentists accept the challenge of such cases, realizing that attempts are typically futile and, in some cases, may create a more unacceptable appearance than the preoperative condition.
The authors will discuss the chemical and physical affects of peroxide on stained tooth structure, the chemical and microphysical process by which teeth lighten in color, and why tetracycline and fluoride staining present a greater challenge. Moreover, we will present a system that has been shown to overcome the challenges of even these most difficult whitening cases, with greater predictability than previously possible.
AGE-RELATED WHITENING CHALLENGES
The “color” of teeth is a result of the wavelengths and amount of reflected light, and encompasses several properties, most notably:
Hue: The specific color; such as blue, green, yellow, red, etc.
Value: The “lightness” or “darkness,” regardless of hue. For example, a black and white photograph shows only variations in value, but shows no hue (color). For the purposes of whitening teeth, our main concern is therefore value.
After removal of extrinsic staining, the visible hue and value (color) of teeth is due to natural pigment within tooth microstructure, as well as intrinsic stain absorbed by tooth microstructure since the time of eruption of the teeth.
Pigment and stain molecules absorb certain wavelengths of light and reflect others, which is responsible for the tooth’s hue and value. A chromophore is a region in a molecule where the energy difference between 2 different molecular orbitals falls within the range of the visible spectrum, and is responsible for its color.
The larger pigment and stain molecules are, the darker they appear. Over time, as patients age, these molecules within the teeth join together, creating larger and larger—and therefore darker and darker—molecules. With time, increasing amounts of intrinsic stain accumulates within tooth microstructure. The combination of accumulation of intrinsic stain and the joining of stain and pigment molecules into larger molecules is responsible for the darkening of teeth that we see with age.
In addition to darkening of teeth, the process of stain absorption into teeth and the joining of these molecules creates a tightly-packed network of stain and pigment molecules within the microstructure of teeth, making it much more difficult for oxygen molecules (ions and radicals released from peroxides) to thoroughly penetrate the tooth’s micro-structure. The result seen by all practitioners is an increasing difficulty in the ability to whiten teeth as patients age.
PHYSICAL AND CHEMICAL PROCESSES CAUSING WHITENING
 |
|
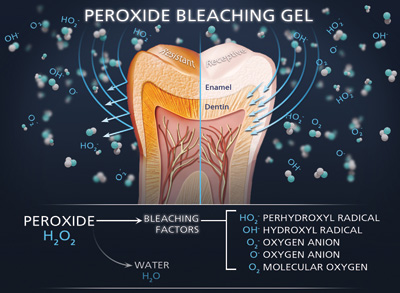
Figure 1. Degradation of hydrogen peroxide (H2O2) into water and bleaching factors: molecular oxygen, double and single anionic oxygen, and free radicals. The ability of tooth structure to absorb bleaching factors determines the predictability of whitening. |
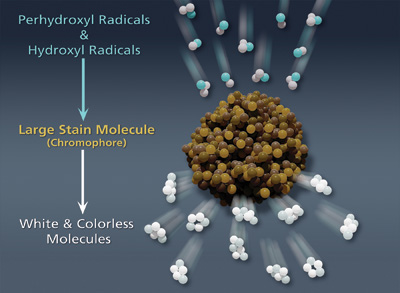 |
| Figure 2. Free radical bleaching factors from H2O2 attack dark, long-chain stain and pigment molecules, breaking them down to tiny colorless and white molecules. |
All peroxide whitening formulations result in an active ingredient of hydrogen peroxide (H2O2). Breakdown of H2O2 results in the release of water (H2O) and “bleaching factors” including molecular oxygen, oxygen ions, and free radicals (Figure 1).
There are 2 distinctly different processes that result from the release of bleaching factors. The first process is oxygenation. The active oxygenation process causes physical and chemical breakdown of stain and debris into smaller particles, and physical removal from tooth structure via diffusion. Not only does this remove some of the stain molecules from tooth structure, causing a lightening of teeth, but it opens the way to allow deeper penetration of tooth microstructure by bleaching factors and removal of more and more debris and stain.
The second process of whitening is the breakdown of deeper, large, long-chain dark stain and pigment molecules by free radicals. Radicals attack unsaturated double bonds of the chromophores, breaking the large molecules down to multitudes of small molecules. The chromophores lose their coloring capacity, and these numerous tiny molecules appear either colorless or white (Figure 2).
Predictable whitening is therefore dependent upon the ability of bleaching factors to penetrate deeply within the microstructure of teeth. Dentists commonly find that single-visit in-office power bleaching of all types has a high incidence of unpredictability, even when perfect technique is utilized. Few dentists have understood why this unpredictability exists.
When the microstructure of the patient’s teeth is not permeable to the low molecular weight bleaching factors, single-visit in-office power bleaching will have minimal effect. Substantial continuous time is necessary for the effective removal of microdebris via oxygenation. If the pathways into the microstructure cannot be cleared, the free radicals are unable to break down the large, long-chain dark stain and pigment molecules.
Dentists who perform whitening procedures on patients in their middle teens typically find that the teeth become amazingly white in a relatively short time. Conversely, dentists who perform whitening procedures on geriatric patients typically find it extremely difficult, and often impossible to achieve an acceptable result.
As patients age, debris accumulates within the microstructure of teeth, within and between enamel rods. Over time, this debris becomes so tightly packed within tooth microstructure that even the low molecular weight bleaching factors are unable to readily penetrate the microstructure.
PERMEABILITY OF BLEACHING FACTORS DETERMINES SUCCESS
Permeability of tooth microstructure to bleaching factors is the primary determinant of how successful the whitening process w
ill be. If bleaching factors have free access and adequate time to saturate the microstructure of teeth, causing removal of debris and stain, and causing the conversion of large, dark long-chain stain and pigment molecules to small colorless or white molecules, whitening will be remarkably successful.
The process of oxygenation is capable of removing significant portions of debris built up within tooth structure; however, it is a time-consuming process. Though high in peroxide concentration, single-visit in-office power bleaching, with 15 to 45 minutes of contact time, does not provide adequate time for removal of debris. Regardless of brand or strength of peroxide, if the bleaching factors released are unable to penetrate the microstructure of teeth, other than temporary dehydration, very little whitening will be accomplished.
Most dentists are aware that conventional at-home bleaching trays provide significant activity for only 25 to 35 minutes. This too is an inadequate amount of time to accomplish thorough removal of accumulated microdebris from tooth structure. The short duration of action when using conventional bleaching trays is due to the loss of bleaching gel from the trays, and especially contamination from ingress of saliva and sulcular fluid into the bleaching trays.
Constant ingress of saliva and sulcular fluid into bleaching trays rapidly inactivates whitening gels. The initial area of saliva/sulcular fluid contamination is at the margin of the bleaching trays, affecting the bleaching gel in the cervical area of the teeth first. This is one of several reasons that cervical portions of teeth are the most difficult to whiten.
There have been recommendations of overlapping the gingival margin with bleaching trays to create a better seal; however, dentists using this method typically find similar problems, as well as more irritation of the gingival margins. By overlapping the gingival margins, the constant secretion of sulcular fluid from the gingival crevice is directed immediately into the cervical portion of the bleaching tray, again quickly deactivating the gel within the tray.
In utilizing the KöR Whitening Deep Bleaching system (Evolve Dental Technologies), developed by Rod Kurthy, DMD, the authors have found an answer to the inconsistencies found with both whitening predictability and sensitivity.
DEEP BLEACHING TECHNIQUE PROTOCOL
 |
|
Figure 3. KöR Deep Bleaching Trays (Evolve Dental Technologies). Note obvious precision fit, as well as the cervical seal (compression of tray against cervical tooth structure). |
The KöR Whitening Deep Bleaching system involves taking and pouring highly detailed impressions that include the facial and lingual gingival crevices throughout each arch. From these detailed models, unique Deep Bleaching Trays (Evolve Dental Technologies) designed to seal bleaching gels in and seal saliva and sulcular fluid out (Figure 3) are fabricated for 2 in-office whitening sessions, and at-home whitening.
The first in-office visit is referred to as the “conditioning visit,” meant to start the process of conditioning (oxygenation debridement) of the microstructure of the teeth. The conditioning visit utilizes 9% hydrogen peroxide with an exceptionally strong chemical accelerator, resulting in release of bleaching factors equal to much higher strength peroxide. With the 9% chemistry, retractors and paint-on dam are not necessary, and the gel is simply delivered in the Deep Bleaching Trays for a total of 40 minutes.
Patients then wear the Deep Bleaching Trays at home for 2 weeks, utilizing a nonaccelerated 16% carbamide peroxide. Given the physical seal of the bleaching trays, the bleaching gel is contained within the trays, effectively sealing out saliva and sulcular fluid. With the seal of the trays, the carbamide peroxide gel does not require the ultra-high viscosity or anhydrous nature of other gels to keep it in the trays. The lower viscosity and 100% aqueous nature of the gel allows a more thorough release of bleaching factors. The seal and chemistry of the bleaching gel provides an extended effective release time of more than 6 hours (some activity has been shown up to 10 hours) instead of the common 25 to 35 minutes of conventional bleaching trays and gels.
The authors have found that Deep Bleaching Trays fit very precisely, resulting in extreme comfort. Most patients wake up in the morning having forgotten the trays are still in their mouths. The seal of the trays also prevents adverse patient reactions seen when viscous gels leak into the mouth while patients are trying to sleep. We have found that the comfort and prevention of rapid leakage of bleaching gels into the mouth have totally overcome patient objections to sleeping with the whitening trays.
When patients present for the final in-office visit, the authors have found a level of whiteness that we have never seen from whitening procedures before. Not only are the teeth significantly whitened, but the conditioning of the teeth (enhanced permeability to bleaching factors) is now complete. Teeth have been rejuvenated to a youthful ability to rapidly absorb bleaching factors, similar to when the patients were teenagers.
The final in-office visit utilizes a high concentration, chemically accelerated 27% hydrogen peroxide. Restoration of the tooth’s youthful ability to absorb the ultralow molecular weight bleaching factors results in the higher concentration hydrogen peroxide’s ability to now flood any remaining resistant chromophores, creating whiteness we have not been able to achieve previously.
BLEACHING RESISTANT FLUORIDE AND TETRACYCLINE STAINS
Fluoride (fluorosis) and tetracycline stains are extremely resistant to conventional whitening. Both stains are more inorganic than other tooth discolorations and very difficult to convert. Both fluoride and the tetracycline family of antibiotics bind strongly to, and become part of, the hydroxylapatite (hydroxyapatite) molecules, which make up the mineral content of enamel, dentin, and bones. They are not simply separate organic stain and pigment molecules to break down.
Fluoride binds with hydroxyapatite, forming fluorapatite, and the tetracycline family bonds (chelates) strongly to hydroxyapatite. These stains have previously been nearly impossible to successfully whiten; however, the ability of the KöR Deep Bleaching System to thoroughly flood the microstructure of teeth with bleaching factors has overcome even these discolorations.
CASE 1: FLUOROSIS
 |
 |
|
Figure 4. Case 1: Preoperative photo of a 22-year-old female with fluorosis demonstrating staining, white and brown mottling. Shown with a VITA C2 shade tab. |
Figure 5. Case 1: Postoperative KöR Deep Bleaching (Evolve Dental Technologies). Shown with the preoperative VITA C2 shade tab. |
 |
| Figure 6. Case 1: Postoperative KöR Deep Bleaching. Shown with postoperative bleaching 020 shade tab. (Shade 020 is more than 3 shades lighter than VITA B1 shade.) |
 |
 |
|
Figure 7. Case 1: Postoperative KöR Deep Bleaching. |
Figure 8. Case 1: Twelve-month postoperative KöR Deep Bleaching. |
The first patient, a 22-year-old female, is also the receptionist of one of the authors. She grew up in a community with a naturally over-fluoridated water supply. The patient presented with heavily mottled teeth (Figure 4). Four previous dentists had refused to attempt whitening, explaining to the patient that whitening would make her appearance even worse. The hypocalcified white spots would whiten excessively, whereas the whitening-resistant background color would not, causing the white spots to become even more noticeable.
The patient was advised that, with the KöR Deep Bleaching System, the white areas would whiten quickly and extremely. However, we also expected the background shade to whiten dramatically, resulting in an overall whiter appearance. It was explained that the white spots would still be visible, but our expectation was that the contrast would be minimized due to effective whitening of the background shade.
The normal KöR Whitening Deep Bleaching protocol was utilized (as described earlier in this article), resulting in an overall whitening result lighter than bleaching shade 020, which is more than 3 shades lighter than VITA shade B1 (Figures 5 and 6). With utilization of the KöR Deep Bleaching System Desensitizers (Evolve Dental Technologies), which occlude dentinal tubules, the patient experienced zero sensitivity throughout treatment.
As you can see in the photographs, the white spots are still present; however, the background shade has whitened so dramatically, the white spots are minimally noticeable (Figure 7), and the patient was extremely happy with the result.
Though the majority of patients would be overjoyed with results such as these, all dentists have encountered patients with unrealistic expectations and a propensity to complain. The authors suggest that, during the preoperative informed consent process, all patients presenting with fluorosis and tetracycline staining be informed that after completion of KöR Deep Bleaching, if more perfection is desired by the patient, restorative or other procedures (microabrasion, composite restorations or porcelain veneers) may be necessary.
The authors have found with utilization of the recommended occasional at-home maintenance, results of KöR Deep Bleaching are entirely permanent, while still allowing patients to continue consuming their favorite foods and beverages such as coffee, tea, and red wine (Figure 8).
CASE 2: TETRACYCLINE STAINING
 |
 |
|
Figure 9. Case 2: Pre-op, 43-year-old male with tetracycline staining. Shown with VITA C4 shade tab. |
Figure 10. Case 2: After 3 weeks of at-home whitening. Shown with VITA C4 shade tab. |
 |
 |
|
Figure 11. Case 2: Post-op KöR Deep Bleaching. Shown with post-op bleaching shade BL4 tab (one shade lighter than VITA shade B-1). |
Figure 12. Case 2: Three-month post-op KöR Deep Bleaching. Shade appears even lighter than the immediate post-op shade. |
The patient is a 43-year-old male with considerable tetracycline staining significantly darker than the VITA C4 shade tab (Figure 9). Several dentists had refused whitening treatment, explaining to the patient that whitening of his teeth was impossible.
The deep bleaching protocol for tetracycline staining is slightly different. Instead of 2 weeks of at-home whitening, 4 to 8 weeks is recommended, depending on the severity and resistance of the case. In the case discussed here, the patient whitened at home for 5 weeks. The patient was seen after 3 weeks of at-home whitening to evaluate his progress. Even at 3 weeks, there was considerable improvement in the shade of the teeth (Figure 10).
Utilizing the same system desensitizers, the patient felt no sensitivity throughout the treatment, up and to the final visit. After the final visit, the patient stated that he may have felt very slight sensitivity, but was not even certain that he had felt any sensitivity at all.
Following the final in-office deep bleaching visit, the patient’s teeth had whitened from a shade considerably darker than shade C4 to lighter than shade BL4, more than one shade lighter than VITA shade B1 (Figure 11).
The patient’s reaction and excitement regarding the results was extreme. The patient was placed on the recommended at-home maintenance and, at a 3-month postoperative visit, it was apparent the shade of the patient’s teeth was even lighter than seen immediately postoperatively (Figure 12).
CONCLUSION
All Whitening Patients Desire Truly White Teeth
Though the author
s have found the KöR Whitening Deep Bleaching System to be profoundly effective in treating otherwise resistant whitening cases, the majority of cases treated with the system are average patients requesting whitening. We have found that patients requesting white teeth have high expectations and respond extremely well to the levels of whiteness achieved by deep bleaching. Moreover, we have found an excessive number of referrals from patients having completed deep bleaching, often including patients who previously were dissatisfied with whitening results achieved from other local practitioners. In addition, we have found that patients who achieve exceptional whiteness of their teeth become much more aware of their smiles. They often become concerned about imperfections that they had not been concerned about, and often had not even previously noticed. The conversion rate of whitening patients to patients requesting additional cosmetic procedures has been very evident and, of course, has greatly affected the bottom-line profitability of our practices.
Predictability of whitening has positively affected the attitude of the dental staffs of our practices. Our team members, who previously were apprehensive to promote whitening (due to the extreme unpredictability), have become excited and aggressive in discussing KöR Whitening Deep Bleaching with our patients.
Dr. Cloud is a 1983 graduate of the University of Tennessee College of Dentistry. He maintains a solo private general practice in Little Rock, Ark. He has earned Mastership in the Academy of General Dentistry, is a Fellow of the American College of Dentists, and a Fellow of the International College of Dentists. He has lectured for the Academy of General Dentistry. He has also been active in providing sports dentistry and has been the team dentist of numerous athletic teams. He can be reached at (501) 868-3800.
Dr. Weibling is a 2001 graduate of The Ohio State School of Dentistry. He attended a general practice residency at St. Elizabeth Hospital in Youngstown, Ohio, from 2001 to 2002. He maintains a solo private practice focusing on complete family dentistry and cosmetic dentistry in Canfield, Ohio. He can be reached at (330) 533-1961.
Disclosure: Drs. Cloud and Weibling report no conflicts of interest.


