
Written by: Drs. Isaac Tawil and Adam Frounfelter
Immediate, full-arch implant surgery has advanced significantly in recent years. What was once a highly analog, technician-driven process involving intraoperative denture conversion has evolved into a sophisticated, digitally guided workflow. Today, clinicians can perform extractions and necessary bone reduction, place implants, capture digital records, and initiate the design of a full-arch prosthesis all within a single surgical session.1 The outcome is faster, more predictable, and often more aesthetic. However, the workflow still presents technical challenges, especially during the capture of intraoral scans in a surgically compromised environment.2
Two recurring problems remain at the heart of the issue. First, intraoral scanners struggle in the presence of blood, soft tissue movement, and pooled fluids.3 The chaotic nature of the surgical field compromises scan accuracy and repeatability.4 Stitching errors and missing data points are common, and exacerbated when scanning identical, often shiny, geometries like healing collars or scan bodies.5 Second, the placement of fiducial markers in hard-to-reach posterior or palatal areas further complicates scanning.6 Traversing flapped tissue to capture these reference markers while maintaining the correlation between them and the multi-unit abutments (MUAs) adds a layer of difficulty that many teams find unpredictable, frustrating, and time-consuming.
To overcome these challenges, a fully integrated, multi-geometric fiducial system, Scanguide, has been developed. This approach enables a single intraoral scan to reference implant positions to the preoperative design without the need for day-of-surgery, pre- and post-surgical scans, or complex postoperative data stitching. When treatment is planned with guided surgery, the fiducial is preplanned in software in the form of a bone reduction guide and Scanguide, stabilized with traditional guide pins. Because the guide’s position is digitally known relative to the teeth, it becomes a fixed reference point through the entire workflow from surgical execution to software prosthetic design.
The advent of these preplanned fiducial systems marks a shift from “reactive scanning” to “proactive record engineering”. No longer must the team work around an unpredictable surgical field to attempt a correlation between implant positions and tooth-based reference data. The surgical guide and fiducial are merged into a single platform, with known digital coordinates and consistent real-world positioning. In this way, the scan becomes a process of verification, not approximation.
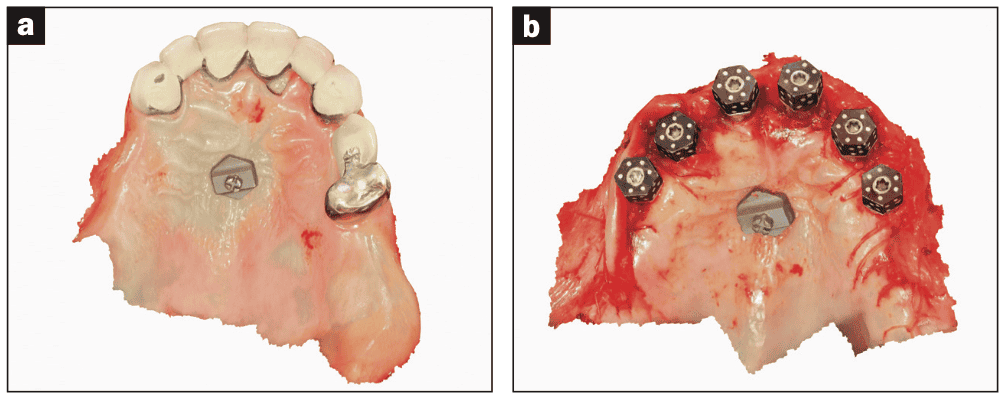
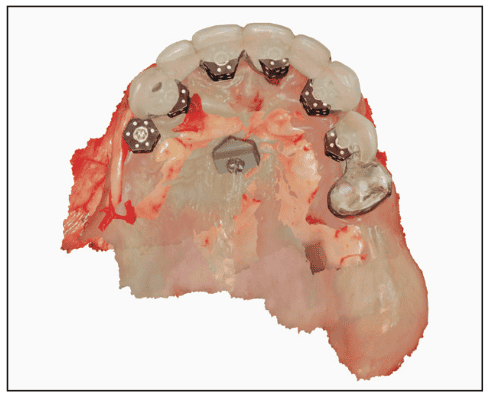
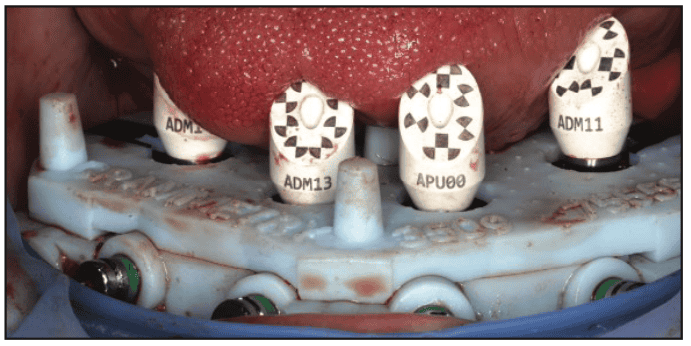
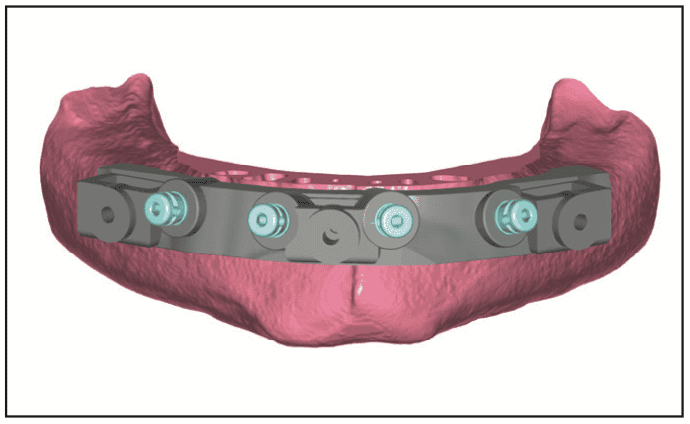
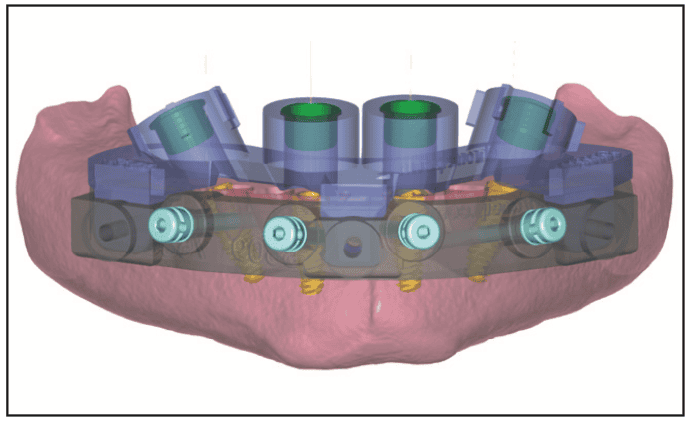
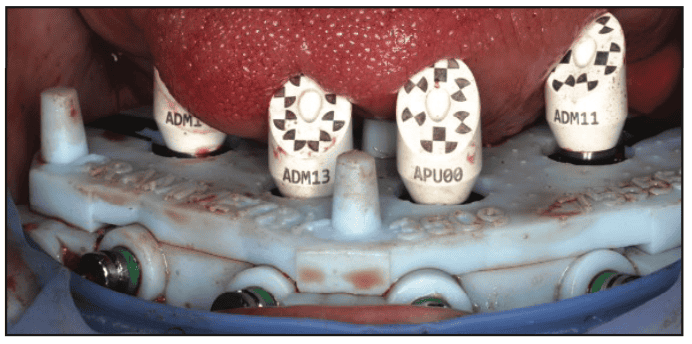
Digital full-arch workflows rely on a variety of fiducial marker strategies.7 These include bone screws or specialty devices placed in the palate or retromolar pad, retained teeth, or complete denture prostheses. In the first 2 types, the intention is to provide a constant landmark that exists in both the pre-op and post-op scans, with the exception of the denture, which is used as a post-op tool to “pick-up” specific landmarks and create the bite and tooth position. The marker workflow typically begins with a presurgical scan capturing the teeth, vestibules/palate, and fiducial (Figure 1a). After extractions, implants are placed, and MUAs are seated. A second scan is then captured either with scan bodies or healing collars (Figure 1b) to include the same fiducial, allowing the technician to align the 2 fiducial markers to register the bite, then design the prosthesis (Figure 2).
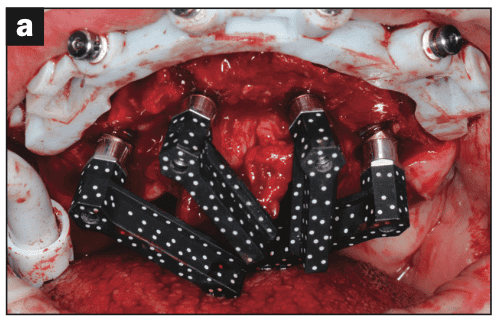
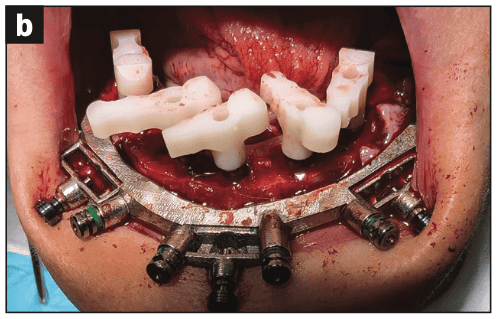
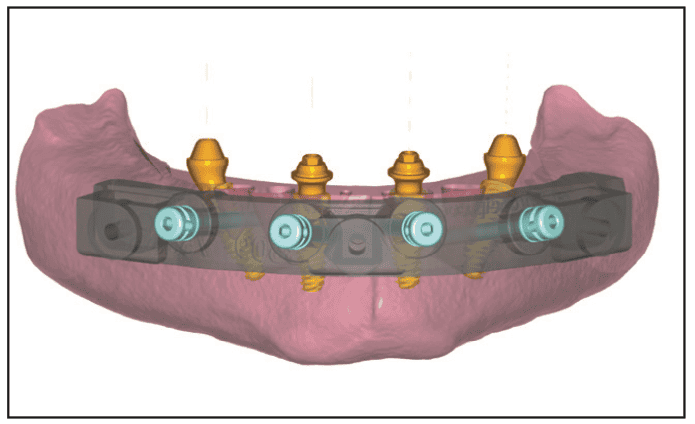
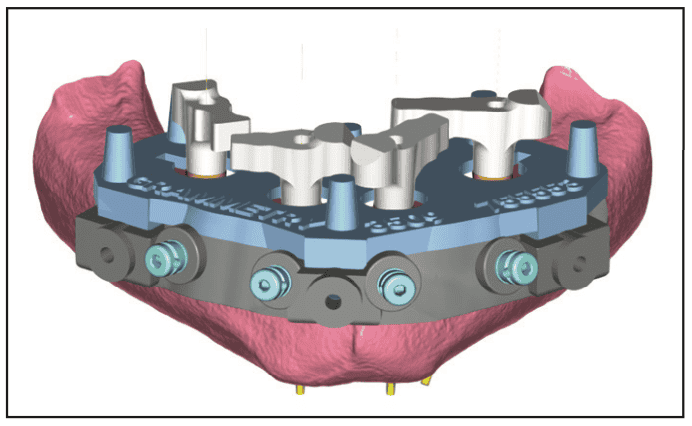
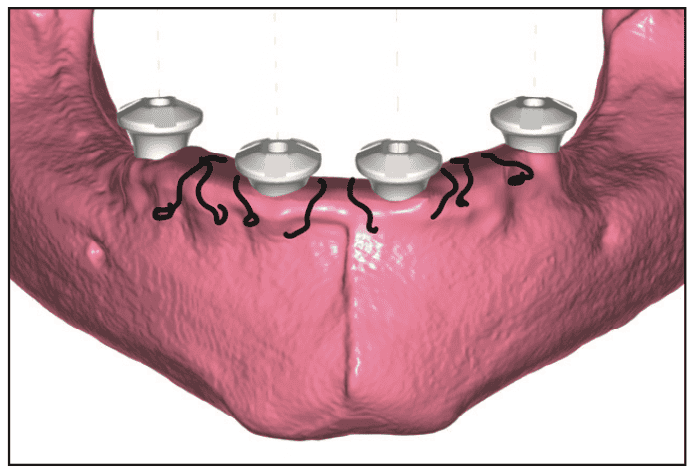
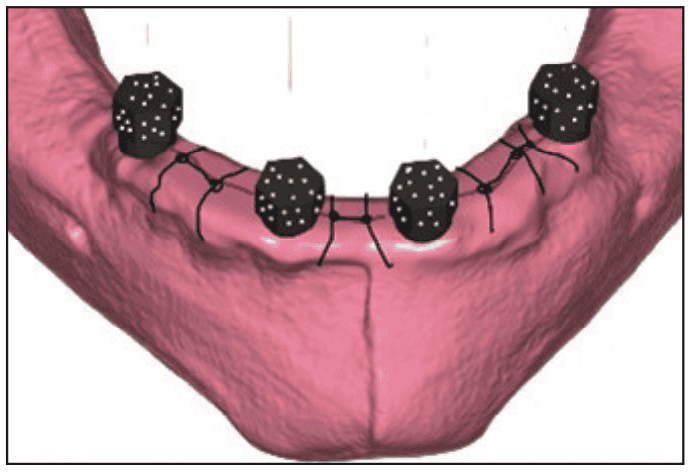
Capturing the challenging scans of the fiducial marker(s), teeth, bite, and bloody tissues is just one part of the equation. The clinical team must also capture the implant/MUA positions in conjunction with the teeth and bite. This is where the issues magnify. Today, the primary MUA capture tools are photogrammetry systems,8 IPG (intraoral photogrammetry), and grammetry (Figures 3 and 4). These tools provide accurate coordinate files of scan bodies connected to the MUAs, which must be correlated to the IOS scans in a third-party software.8 This registration of 2 data sets is complex, and the quality of the final alignment relies heavily on the quality of the IOS scans and, in turn, the technician’s skill. Grammetry offers a unique approach of allowing the user to capture the MUA positions and the fiducial markers in one scan and necessitates additional registration to the teeth and bite. In both workflows, IOS scanning accuracy is critical.
In contrast, IPG systems like SHINING 3D’s Aoralscan Elite deliver both the implant coordinates and intraoral scan data in a single pre-aligned file, streamlining the correlation and reducing the potential for error. However, even IPG requires a stable reference to ensure alignment with the digital wax-up or original tooth position.
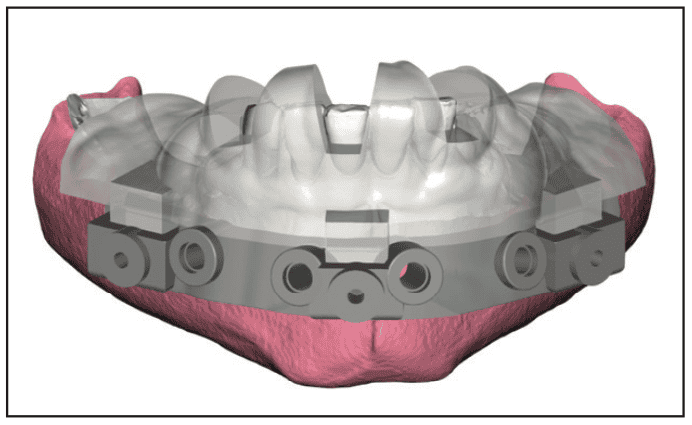
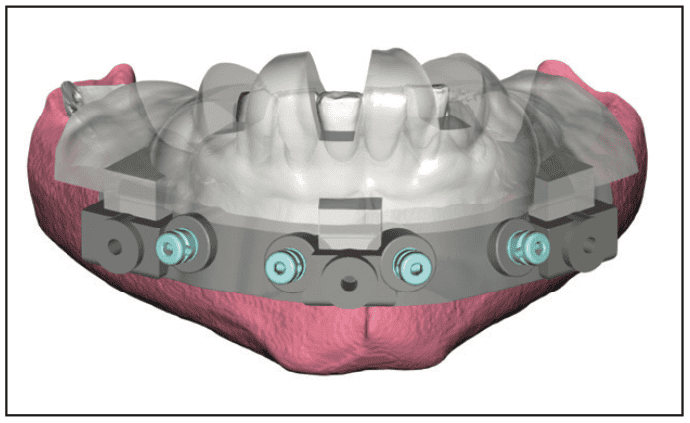
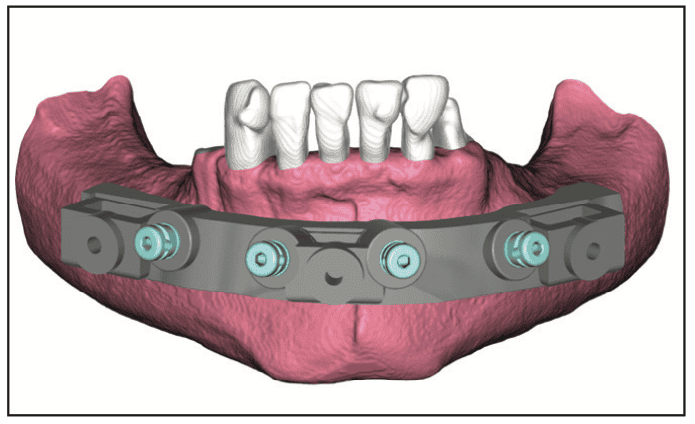
This is where the Scanguide’s “one-scan technique” (Figures 5 to 15) offers a dramatic improvement. Because the fiducial system is digitally designed and integrated into the surgical guide, its position is already relative to the teeth, wax-up, bite, and opposing are already known (Figure 4). The occlusal masking platform, fabricated in a scannable material and engineered with unique geometries, provides a masking surface around the MUAs to block out the hard-to-scan surfaces. When placed over the healing collars or scan bodies (Figure 13), the platform guides the scanner and allows for a single, accurate scan that captures both the fiducial and the MUA components.

This approach eliminates the need for a presurgical fiducial scan, as the preplanned fiducial system has been designed in conjunction, and integrated with, the implant plan design and surgical guide manufacture. The clinician need only capture the interoperative MUA positions relative to the marker, and this one file is brought back into the ‘stack’ for prosthesis design.
In our workflow, we have implemented this system through the GuidedSMILE digital product called CombiGuide, developed with ROE Dental Laboratory. This guide comes in 2 versions: a labial bone reduction guide only (Step 3a, Figure 7), or a bone reduction guide with an osteotomy guide (Step 4a, Figure 9). Both include a scannable masking platform, which serves to block out the tricky scanning services mentioned above. The reduction guide and the scan platform are used as the fiducial markers and have proven to be especially valuable in immediate load cases, where time is critical and precision is essential.
The benefits of this approach are broad. First, it removes one of the most error-prone steps in full-arch workflows, the intraoperative scan. By replacing difficult scan zones with a purpose-built platform, clinicians can reliably capture the necessary data in seconds and not be frustrated by lost IOS scans. Second, it improves the quality of provisional prosthetics because the design is based on a pre-op wax-up aligned to the marker. Predetermined bone reduction, implant positioning, morphology, and occlusion can be better controlled. Emergence profiles, midline, and aesthetic principles are preserved through to the final, and bite openings are performed before surgery in a lab-controlled environment, rather than in software, post surgery.
This system also improves interdisciplinary communication. Because the marker is common to both the surgeon and the restorative team, everyone is working from the same digital map. There is no longer a disconnect between surgical execution and lab interpretation. That level of coherence improves confidence across the team and leads to better outcomes at delivery.
From a patient standpoint, the experience is smoother and more efficient. Surgery is completed in less time, with fewer surprises. Provisionals are more comfortable and better fitting. There are fewer post-op appointments for bite correction or flange trimming. And most importantly, the patient leaves with a result that reflects the original design rather than an improvised chairside conversion.
The integration of preplanned fiducials and scannable platforms is not just a technical enhancement; rather, it is a strategic shift in how we approach full-arch implant dentistry. By controlling the surgical record at the point of data acquisition, we eliminate variability, reduce turnaround, and improve the final prosthetic result. Whether using intraoral or extraoral photogrammetry or IOS grammetry, this protocol offers a unified, simplified, and clinically robust method for capturing digital records.
This approach reflects a broader evolution in full-arch workflows, one that prioritizes verifiable data acquisition at the time of surgery. As digital protocols continue to mature, we can expect further refinement in scan materials, platform geometry, and software integration. Still, the foundation remains unchanged: predictable prosthetic outcomes begin with accurate surgical records. By anchoring the digital workflow to a stable, known reference point, clinicians can streamline communication with the restorative team, reduce errors, and enhance the overall quality of care delivered to the patient.
The One-Scan Technique: Clinical Efficiency Reimagined
What truly defines the value of this approach is its capacity to collapse what was once a multi-step protocol into a single, unified capture event. Known as the “one-scan technique,” this method is rooted in surgical simplicity and digital precision. By relying on a single intraoral scan that contains the reference marker and the prosthetic components including healing collars, scan bodies, or photogrammetric markers, clinicians eliminate the layered scanning protocols that have traditionally required significant effort, time, and technical dexterity. The process no longer demands separate scans for the pre-op condition, the post-extraction anatomy, and the final implant positions. Instead, the full digital context is captured in one controlled moment, making the workflow both faster and more reliable. This unified capture not only simplifies the procedure for the clinician but also strengthens the quality of the data received by the laboratory, ultimately elevating the precision of the prosthetic outcome.
The reduction of scanning complexity is particularly impactful when managing sedated or medically compromised patients. Traditional workflows often require a pre-op scan, followed by a scan post-extraction, and then another after implant placement followed by a sutured tissue scan—all while the patient is under anesthesia. Each added scan increases time, introduces movement, and requires team coordination. With the one-scan technique, once the surgical portion is complete and the platform is secured, a single scan suffices. This not only reduces chair time but minimizes patient discomfort and the risks associated with prolonged sedation. The streamlined process also allows the surgical and restorative teams to focus on accuracy and patient care, rather than troubleshooting scan inconsistencies or realigning mismatched datasets. As a result, outcomes are not only more predictable but also achieved with less stress and greater clinical confidence.
From a training and scalability perspective, the implications are equally important. Many clinicians, particularly those entering full-arch rehabilitation for the first time, find the most intimidating aspect to be the technical overlap between surgery, scanning, and prosthetic planning. By unifying the process under a simplified protocol, new users can reliably reproduce results with less dependence on highly skilled digital assistants. This democratizes access to digital full-arch workflows and removes many of the barriers that previously limited widespread adoption. It also facilitates smoother onboarding of new team members, allowing practices to grow without being bottlenecked by a few key individuals. Ultimately, it encourages more clinicians to offer immediate load solutions with confidence, knowing that the workflow is repeatable, supported by digital tools, and built around a verified reference point that guides every phase of treatment.
Eliminating the presurgical scan may also reduce cognitive load during planning. Since the reference marker is designed directly into the surgical guide, the digital technician no longer requires presurgical IOS data for alignment. This means surgical planning, digital wax-ups, and implant positions can all be designed from a single virtual model centered around the marker. This model then becomes the reference for everything that follows, including the post-op prosthetic scan.
Another essential benefit lies in how the technique strengthens the restorative chain of trust. For years, labs have had to navigate inconsistent scans, shifting bite records, or questionable scan body positioning. When scan data and implant coordinates are built around a digitally anchored reference, the likelihood of distortion or misalignment is dramatically reduced. The scan becomes the most reliable link in the workflow, not the most vulnerable one.
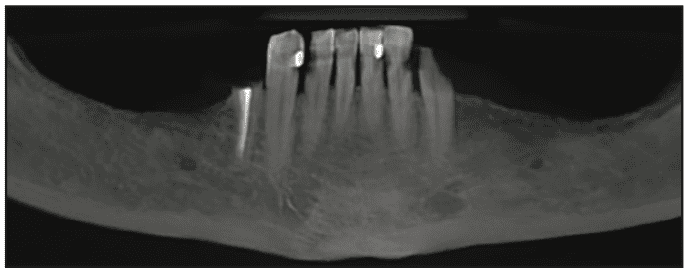
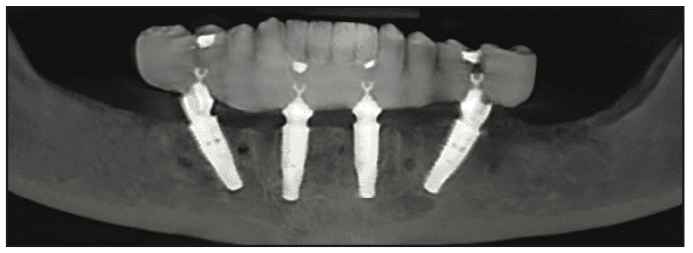
From a prosthetic design standpoint, the preplanned nature of the workflow also allows for highly controlled emergence profiles and soft tissue shaping. Because the platform geometry encircles the MUAs, the prosthetic team can better visualize how tissue will heal around the provisional and final restorations. The result is improved aesthetic outcomes, reduced risk of inflammation or over-compression, and fewer adjustments during final delivery, as outlined in the step-by-step guide and in pre-op and post-op panoramic x-rays and photos shown in Figures 16 to 19.


Looking ahead, this streamlined protocol aligns perfectly with the future of implant prosthodontics. As artificial intelligence (AI) and automated design tools begin to integrate into prosthetic CAD software, the value of clean, structured input data cannot be overstated. The one-scan technique provides that structure, giving both the human technician and the AI-driven system a clear, unambiguous starting point.
In an industry increasingly driven by efficiency, quality control, and patient experience, the one-scan technique offers a rare convergence: it is faster without cutting corners, more accurate without complexity, and accessible without compromise. Whether implemented in a private practice, institutional program, or full-service surgical center, this approach empowers teams to deliver consistent, aesthetic, and functionally sound outcomes at scale.
REFERENCES
- Ganz SD, Tawil I. Full-arch implant surgical and restorative considerations: utilizing a full template guidance technique. Dent Today. 2019;38(9):72–8.
- Tawil I, Domingue D. Navigating the complexities of digital full-arch implant treatment. Inside Dentistry. 2024;20(6).
- Alkadi L. A comprehensive review of factors that influence the accuracy of intraoral scanners. Diagnostics (Basel). 2023;13(21):3291. doi:10.3390/diagnostics13213291
- Mangano FG, Admakin O, Bonacina M, et al. Trueness of 12 intraoral scanners in the full-arch implant impression: a comparative in vitro study. BMC Oral Health. 2020;20(1):263. doi:10.1186/s12903-020-01254-9
- Tawil I, Ganz SD. Fully digital full arch? Continued advancements in full-arch implant restorations. Dent Today. 2023;43(4).
- Zhao Y, Liao Y, Wu X, et al. Effect of the number and distribution of fiducial markers on the accuracy of robot-guided implant surgery in edentulous mandibular arches: An in vitro study. J Dent. 2023;134:104529. doi:10.1016/j.jdent.2023.104529
- Han YT, Lin WC, Fan FY, et al. Comparison of dental surface image registration and fiducial marker registration: an in vivo accuracy study of static computer-assisted implant surgery. J Clin Med. 2021;10(18):4183. doi:10.3390/jcm10184183
- Jensen OT, Ross D, Jivraj S, et al. Provisional prosthetic outcome when using photogrammetry for complete arch oral implants: a report of 111 patient treatments. Oral Maxillofac Surg Clin North Am. 2024:37(2):179–92. doi:10.1016/j.coms.2024.11.005
ABOUT THE AUTHORS
Dr. Tawil received his DDS degree from New York University College of Dental Surgery and has a masters degree in biology. He is the clinical director of TBS Dental and SHINING 3D, and co-director of CHROME GuidedSMILE. Dr. Tawil is a MINEC Ambassador (Megagen International Network of Educators and Clinicians), Ambassador of Digital Dental Society and The Clean Implant Foundation, a board member of MINEC USA, Digital Dental USA Society, and the Slowdentistry movement. Dr. Tawil is a Diplomat of the International Academy of Dental Implantology and the International Academy for Dental Facial Esthetics. He is a Fellow of the International Congress of Oral Implantologists. He is one of Dentistry Today’s top leaders in CE, a faculty member of the Osseodensification Academy, educational director of Brighter Way in Phoenix, digital director of CHROME GuidedSMILE, and consultant for Glidewell laboratories. Additionally, Dr. Tawil is a recipient of the Pierre Fauchard Award for outstanding achievements in dentistry and the Presidential Service Award. He is the founder of Advanced Implant Education, and a partner in TBS instruments and Universal Shapers LLC. Dr. Tawil has published in several journals, textbooks, and magazines on implantology and digital dentistry. Dr. Tawil has held main podium sessions and hands-on workshops worldwide and enjoys a private practice in Brooklyn, New York. He can be reached at [email protected].
Dr. Frounfelter is a skilled and compassionate dentist who transforms lives through full-arch dentistry. Based in Evansville, Ind, he specializes in same-day smile transformations using a fully digital workflow, including intraoral scanners, CBCT imaging, CHROME GuidedSMILE technology, and photogrammetry—to deliver powerful, precise results with efficiency and excellence. His one-day, full-arch protocol is built on the foundation of a highly trained, empowered team. Every step of his workflow is team-driven, ensuring seamless coordination, elevated patient care, and life-changing outcomes. Known not only for his clinical skill but for his grounded, humble presence, Dr. Frounfelter has a gift for making everyone around him feel valued and important. He can be reached at [email protected].
Disclosure: The authors report no disclosures.



