
Written by: Nadim Z. Baba, DMD, MSD
INTRODUCTION
Fixed prosthodontics plays a principal role in modern restorative dentistry, uniting biological, functional, and aesthetic principles to rehabilitate the dentition. As patient expectations for natural-looking, durable restorations continue to rise, the clinician’s challenge lies in balancing material selection, tooth preservation, tissue management to keep them healthy, and long-term maintenance. Success in fixed prosthodontics depends not only on technical skill but also on comprehensive treatment planning and adherence to biomechanical and biological principles that support the restoration and the surrounding tissues over time.
Contemporary fixed prosthodontics emphasizes minimally invasive tooth preparation and the use of advanced ceramics that mimic natural tooth structures. At the same time, function remains paramount: occlusal stability, proper load distribution, and periodontal health are essential for lasting results. Each clinical step, from diagnosis to definitive cementation, affects the long-term prognosis of the prosthesis. To achieve success, clinicians need to adhere to the basic principles of fixed prosthodontics and plan their cases before they start preparing their teeth.
This article reviews key considerations for restoring aesthetics and function in fixed prosthodontics, focusing on diagnosis and treatment planning, practical guidelines for the selection of ceramic materials, tooth preparation, tissue management, definitive impression, shade selection, provisionalization, cementation, and maintenance. The goal is to help practitioners achieve predictable, long-term outcomes that integrate seamlessly with the patient’s natural dentition.
Diagnostic and Treatment Planning
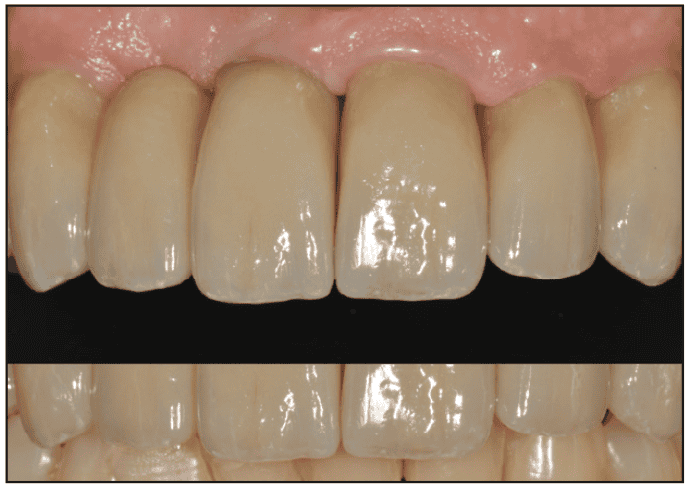
The goal of prosthodontic rehabilitation is to emulate nature. Our aim is to replicate the intricate details and delicate nuances found in natural teeth. Paying attention to these details will allow the clinician to provide the patient with restorations that restore his or her aesthetics and function and help regain a beautiful smile (Figure 1).
Aesthetics is defined as the theory and philosophy that deal with beauty and the beautiful, particularly with regard to the appearance of a dental restoration.1 It is the science of copying our work with that of nature, making our art inconspicuous.2 A survey of patient attitudes toward current aesthetic procedures showed that only 30% to 40% of adults with inharmonious anterior teeth are not satisfied with their smile.3
Aesthetics requires knowledge of facial aesthetics coupled with knowledge of natural tooth position. The most important attractiveness characteristics are general appearance and the face.4 The eyes and the mouth are facial features most commonly associated with facial attraction. They produce emotional expression; they are the moving parts of the face, and they play an important role in recognition.5-8
Facial analysis is a very important step before moving to the details of the teeth. Analysis of the patient’s frontal and lateral views is essential. One of the most important analyses, besides determining the midline and making sure that the teeth are parallel to the interpupillary line, is the amount of tooth display. Tooth exposure ranges from 1 to 5 mm, depending on the patient’s lip height, age, and gender. Women show more teeth at rest than men do, and young patients show more teeth than middle-aged patients. Age can diminish tooth visibility due to tooth abrasion and a reduction of perioral muscle tone. It is crucial to evaluate the maxillary incisors at rest for any restorative treatment. A recent review of research on aesthetics examined the attractiveness of the smile, the effect of aging on the smile, oral condition and the smile, personality and the smile, and smile exercises. When they examined the curvature of the maxillary anterior teeth in relation to the lower lip, they concluded that public preference favored the maxillary lip being parallel to the lower lip (Figure 2). Similarly, the public preferred the maxillary teeth not to touch the lower lip (Figure 3).8


Choice of Ceramic Materials
Ceramic materials have evolved dramatically in the last 2 decades, offering a wide range of options that differ in strength, translucency, and bonding characteristics. The clinician’s challenge is to select a material that balances aesthetics, mechanical demands, and biological compatibility.
Leucite-reinforced and lithium disilicate ceramics exhibit excellent optical properties, closely matching the translucency and light-diffusion properties of natural enamel. Lithium disilicate, in particular, combines superior aesthetics with flexural strength in the range of 400–500 MPa, making it suitable for single crowns and short-span anterior bridges when bonded adhesively. These materials allow conservative tooth preparation due to their bonding capacity but require meticulous bonding protocols and isolation to ensure longevity (Figure 4).

Alumina and zirconia-based ceramics offer high flexural strength and fracture resistance, making them ideal for posterior restorations, implant abutments, and multi-unit prostheses. Monolithic zirconia restorations have improved significantly in translucency, reducing the aesthetic compromise once associated with traditional opaque zirconia cores. However, zirconia’s low glass content limits its etchability, necessitating the use of mechanical retention and resin cements containing phosphate monomers for optimal adhesion (Figure 5).

Ultimately, no single ceramic suits all cases. Understanding the patient’s occlusal scheme, parafunctional habits, and aesthetic expectations guides the optimal selection.
Tooth Preparation Principles
Tooth preparation forms the biological and mechanical foundation for long-term success. The preparation must conserve enamel and dentin while providing adequate space for restorative materials and ensuring a smooth, continuous margin for marginal adaptation.
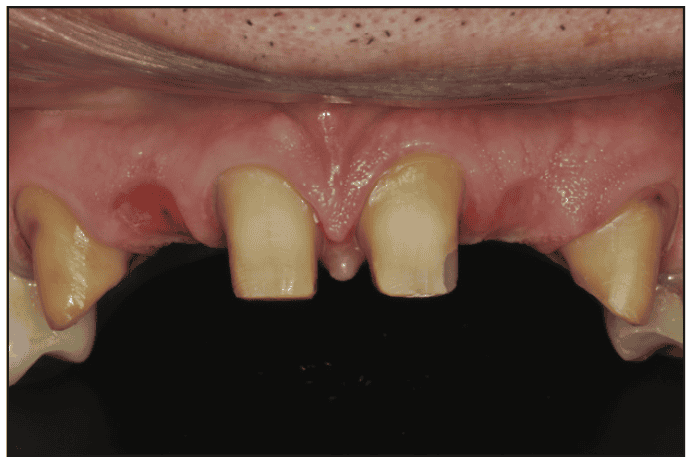
Adhesive materials have reduced the need for extensive mechanical retention. However, proper axial wall taper, ideally between 6° and 10°, remains essential to resist dislodging forces, particularly in posterior regions or when bonding conditions are suboptimal. Over-tapering or undercut formation should be avoided, as these compromise seating and retention (Figure 6).
- The choice of finish line depends on both material type and tissue health. Three finish lines have been used with all-ceramic crowns:
- Shoulders with sharp axiogingival line angles are formed using burs such as a #56L to create a sharp internal angle and then smoothed with a hand instrument.
- Shoulders with rounded axiogingival line angles are formed using diamond instruments with a rounded tip. Care must be taken to eliminate peripheral ridges in the finish lines caused by the round bur.
- A chamfer or deep chamfer is formed using diamond instruments with a rounded or angled end. When placed into the tooth a distance that equals half the instrument diameter, a chamfer finish line is formed as the instrument is moved around the perimeter of the tooth. A chamfer provides adequate bulk for ceramics while minimizing stress concentration. Subgingival margins should be reserved for cases requiring aesthetic masking or caries management (subgingival caries); otherwise, supragingival margins are preferable to facilitate hygiene, impression accuracy, and facilitating hygiene (Figure 7).

To facilitate accurate fabrication of all-ceramic crowns, it is recommended that finish lines not have excessive cervical slope and that there be no abrupt occlusocervical undulations in the finish line. Finish line uniformity and smoothness improve marginal fit. Even smooth reductions prevent internal stress in brittle ceramics and improve adaptation.9 Sharp angles should be rounded to reduce stress risers. Reduction guides or silicone matrices from diagnostic wax-ups help achieve predictable and uniform reduction.
When a proximal restoration is missing or substantial proximal tooth structure is removed due to caries, the tooth should be restored to maintain normal proximal form (well retained by remaining tooth structure). Greater leverage is created on the uneven side of the tooth.
Incisal reduction of 2 mm is required on anterior teeth. It is also recommended that the lingual surface be reduced 1 to 1.5 mm for occlusal clearance with the opposing teeth. Functional cusp reduction must accommodate both material thickness and occlusal dynamics. For lithium disilicate, at least 1.5 to 2.0 mm of occlusal clearance is required; zirconia may allow slightly less due to its higher strength. Occlusal reductions of 2 mm are biologically acceptable even on young teeth due to the available thickness of enamel and dentin on the occlusal surface. Many all-ceramic crown fractures appeared to be related to copings of questionable thickness.10 Ceramic thickness and occlusion were of paramount importance to clinical success. Maintaining the patient’s occlusal vertical dimension and centric relation throughout treatment is essential for functional harmony.
Tissue Management and Definitive Impression
Accurate impressions depend on healthy peri-gingival tissues and effective moisture control. Tissue management is crucial for capturing precise margin detail and ensuring biologic width preservation.
Gingival inflammation must be resolved before impression making. If necessary, the patient can be placed on a regimen of Chlorhexidine for a week prior to definitive impression. Prior to tooth preparation: prepack healthy tissues with nonimpregnated retraction cord (buffer zone) to prevent laceration of tissues during high-speed cutting.
Mechanical retraction using a single- or double-cord technique remains the gold standard for exposing subgingival margins. Cord (braided or knitted) impregnated with hemostatic agents (such as aluminum chloride) aids in fluid control when inserted with a serrated instrument. Do not leave the cords for more than 30 minutes, and when packing the cords, exert normal pressure. Excessive, forceful retraction using multiple cords to make multiple impressions should be avoided.11
Digital impression systems have transformed fixed prosthodontics by offering high accuracy, improved patient comfort, and the ability to integrate with CAD/CAM workflows. For subgingival margins, hybrid approaches, combining cord retraction with intraoral scanning, yield reliable results. For conventional impressions, addition silicone (PVS) and polyether materials remain the standard when meticulous moisture control is used.
Encroachment on the biologic width leads to chronic inflammation and attachment loss. The restorative margin should ideally remain 0.5 to 1 mm supragingival or at the most juxtagingival when aesthetics dictate, always respecting tissue health.
Provisionalization
Provisional restorations serve as diagnostic and protective tools, providing information about aesthetics, phonetics, and function before final restoration. They also preserve pulpal vitality, prevent tooth migration, and maintain soft-tissue architecture.
Provisionals may be fabricated directly in the mouth or indirectly. Indirect or digitally fabricated provisionals generally offer superior fit, contour, and polishability, reducing chairside adjustments and gingival irritation. Bis-acryl composite resins have been frequently used. However, for extensive and long-term restorative rehabilitations (full-arch or full-mouth rehabilitations) on natural teeth or implants, PMMA milled provisionals have become the material of choice due to their strength, marginal integrity, and polishability (Figure 8).

Provisional restorations allow clinicians to test occlusal relationships, incisal edge position, and emergence profiles, phonetics, and aesthetics. Adjustments made at this stage can guide the definitive restoration design. When provisionalizing multiple units, splinting may be necessary to achieve stability, particularly when abutments are compromised.
Proper contour and emergence of provisionals can sculpt soft tissues to the desired gingival profiles. Over-contoured or grossly under-contoured provisionals and surface roughness can compromise tissue health, emphasizing the importance of anatomic contouring and polished margins.12-14
Cementation
The final cementation step unites biological, mechanical, and material considerations. The choice of cement and technique depends on the restorative material, retention form, and clinical environment.
Cements can be broadly divided into conventional and adhesive resin cements. Conventional, glass-ionomer, resin-modified glass-ionomer (RMGIC), or self-adhesive resin cements (SAC) are indicated when mechanical retention is strong and moisture control is challenging. Many manufacturers recommend air-particle abrasion before cementation, especially with self-adhesive resin cements, to improve bond strength.
For glass-ceramic crowns, etch the intaglio surface of the crown with hydrofluoric acid (5% to 10%) followed by silane coupling agent application. For zirconia crowns, air-particle abrasion (sandblasting) with aluminum oxide (30-50 µm) and MDP-based primers provide the highest bond strength between RMGIC and zirconia.15
After try-in, clean the restoration in an ultrasonic cleaner, a cleaning bath, and alcohol for 5 minutes, or use a zirconia/ceramic cleaner. Condition the tooth with a mild solution of polyacrylic acid, apply cement, and seat the crown. Rubber dam isolation ensures optimal results, though alternatives such as retraction cords and absorbent isolation may be acceptable in posterior regions. Riva Cem Automix cement (SDI) is an RMGIC, a self-curing, radiopaque releasing paste indicated for permanent cementation of metal-based and strengthened-core ceramic restorations (Figure 9). This cement is excellent for cementation of crowns made of zirconia, lithium disilicate, feldspathic porcelains, and glass ceramic. When compared to other similar cements, Riva Cem Automix has an excellent bond strength to both enamel and dentin. In addition, it has high compressive and flexural strength, and the most important factor is that it has the least waste due to its small tip. RMGIC is my cement of choice for zirconia crowns.
After cementation, all excess cement should be promptly removed to avoid gingival irritation and secondary caries. Occlusal contacts and proximal relationships should be rechecked to prevent premature contacts or food impaction.
Maintenance
Long-term success in fixed prosthodontics depends heavily on regular maintenance and patient cooperation. Even the most technically perfect restoration can fail prematurely if biological or mechanical complications are not prevented. Regular recall appointments (typically every 6 months) allow for evaluation of marginal integrity, tissue health, and occlusal stability. Periodontal probing and radiographic monitoring help detect early signs of secondary caries, marginal leakage, or cement dissolution.
Patients should be instructed on meticulous oral hygiene, including the use of interdental brushes, floss threaders, or water flossers around bridge pontics and abutments. Nightguard use is strongly advised for patients with bruxism or parafunctional habits to protect ceramic restorations from fracture.
Minor ceramic chipping can often be repaired intraorally with composite resin and silane coupling agents, thereby prolonging the life of the restoration. However, repeated fractures or debonding often indicate occlusal overload or improper material selection and require comprehensive reevaluation.
CONCLUSION
Restoring aesthetics and function through fixed prosthodontics requires a balance of art and science. Long-term success depends on a continuum of decisions, from material selection and tooth preparation to cementation and maintenance, each affecting biological harmony and mechanical stability.
Modern ceramics and adhesive technologies have expanded the clinician’s ability to deliver restorations that are both conservative and highly aesthetic. However, these advances demand precise execution of clinical protocols, adherence to evidence-based principles, and commitment to ongoing maintenance.
Ultimately, successful fixed prosthodontics is not defined solely by the appearance of the final restoration but by its integration with the patient’s oral environment, preserving health, comfort, and confidence for years to come.
REFERENCES
1. The Glossary of Prosthodontic Terms: Ninth Edition. J Prosthet Dent. 2017;117(5S):e1-e105. doi:10.1016/j.prosdent.2016.12.001
2. Pilkington EL. Esthetics and optical illusions in dentistry. J Am Dent Assoc. 1936;23(4):641–51.
3. Goldstein RE, Lancaster JS. Survey of patient attitudes toward current esthetic procedures. J Prosthet Dent. 1984;52(6):775–80. doi:10.1016/s0022-3913(84)80001-3
4. Lerner RM, Karabenick SA, Stuart JL. Relations among physical attractiveness, body attitudes, and self-concept in male and female college students. J Psychol. 1973;85(1st Half):119–29. doi:10.1080/00223980.1973.9923870
5. Secord PF, Dukes WF, Bevan W. Personalities in faces. I. An experiment in social perceiving. Genet Psychol Monogr. 1954;49(2):231–79.
6. Galper RE, Hochberg J. Recognition memory for photographs of faces. Am J Psychol. 1971;84(3):351–4.
7. Sorce JF, Campos JJ. The role of expression in the recognition of a face. Am J Psychol. 1974;87(1-2):71-82.
8. Dong JK, Jin TH, Cho HW, et al. The esthetics of the smile: a review of some recent studies. Int J Prosthodont. 1999;12(1):9-19.
9. Walton CB, Leven MM. A preliminary report of photoelastic tests of strain patterns within jacket crowns. J Am Dent Assoc. 1955;50(1):44–8. doi:10.14219/jada.archive.1955.0003
10. McLaren EA, White SN. Survival of In-Ceram crowns in a private practice: a prospective clinical trial. J Prosthet Dent. 2000;83(2):216–2. doi:10.1016/s0022-3913(00)80015-3
11. Baba NZ, Goodacre CJ, Jekki R, et al. Gingival displacement for impression making in fixed prosthodontics: contemporary principles, materials, and techniques. Dent Clin North Am. 2014;58(1):45-68. doi:10.1016/j.cden.2013.09.002
12. Chiche G. Improving marginal adaptation of provisional restorations. Quintessence Int. 1990;21(4):325–9.
13. Orkin DA, Reddy J, Bradshaw D. The relationship of the position of crown margins to gingival health. J Prosthet Dent. 1987;57(4):421–4. doi:10.1016/0022-3913(87)90006-0
14. Newcomb GM. The relationship between the location of subgingival crown margins and gingival inflammation. J Periodontol. 1974;45(3):151–4. doi:10.1902/jop.1974.45.3.151
15. Alnassar T, Ozer F, Chiche G, et al. Effect of different ceramic primers on shear bond strength of resin-modified glass ionomer cement to zirconia. J Adhes Sci Dent. 2016;30(22):2429–38. doi:10.1080/01694243.2016.1184404
ABOUT THE AUTHOR
Dr. Baba received his DMD from the Université de Montréal in 1996. He completed a certificate in Advanced Graduate Studies in Prosthodontics and a master’s in Restorative Sciences in Prosthodontics from Boston University School of Dentistry in 1999. Dr. Baba serves as a professor in the advanced education program in implant dentistry at Loma Linda University School of Dentistry, an adjunct professor at the Boston University Goldman School of Dental Medicine department of Restorative Sciences and Biomaterials, and maintains a part-time private practice in Glendale, Calif. He is the past president of the American College of Prosthodontists, an active member of various professional organizations, and a Diplomate of the American Board of Prosthodontics, a Fellow of the American College of Prosthodontists, and a Fellow of the Academy of Prosthodontics.
He is also a reviewer for the Journal of Prosthetic Dentistry, an associate editor for the Journal of Prosthodontics, section editor for Prosthodontics in the Journal of Esthetic and Restorative Dentistry, and was the associate editor for the Aesthetics/Prosthetics/Restorative section at the Journal of Dental Traumatology for 11 years. Dr. Baba has received several honors and awards including: The David J. Baraban Award from Boston University, the Claude R. Baker Faculty award for Excellence in Teaching Predoctoral Fixed Prosthodontics in 2009 from the AAFP, the California Dental Association Arthur A. Dugoni Faculty award in 2010, and the Robert James Achievement Award from the Advanced Education Program in Implant Dentistry at Loma Linda University in 2025. He is the author of numerous publications and has lectured nationally and internationally. He can be reached at [email protected].
Disclosure: Dr. Baba received an honorarium from SDI for writing this article.



