Influenza (“the flu”) is a contagious respiratory illness caused by 2 types of influenza viruses. Symptoms range from mild to severe with life-threatening complications. On average, 114,000 people are hospitalized for flu-related complications each year. More than 36,000 people in the United States die annually because of influenza. Hospitalizations and deaths are most common among those greater than 65 years, young children, and all ages with underlying health conditions such as congestive heart failure, asthma, or diabetes.1,2
In the United States, winter is the time for flu. The flu season can range from November through March and even past March in some years. During the past 21 flu seasons, the heaviest flu activity (peak month) occurred in February (Table 1).
| Table 1. Peak Months of Flu Activity (Over the Last 21 Years).* |
 |
| *Modified from Reference 2 |
SYMPTOMS OF FLU
Symptoms of flu include fever (usually high), headache, extreme tiredness, dry cough, sore throat, runny or stuffy nose, and muscle aches and pains. Gastrointestinal symptoms, such as nausea, vomiting, and diarrhea, are much more common among children than adults. Sometimes the term “stomach flu” is associated with gastrointestinal symptoms (“sick to your stomach”). These illnesses are not often related to influenza viruses, but rather to other viruses, bacteria, or even parasites. Flu is a respiratory disease, not a stomach or intestinal affliction.1-3
The flu and the common cold are both respiratory illnesses caused by different viruses that often develop at the same time of year. Because these 2 types of illnesses have similar symptoms, it can be difficult to tell the difference between them. In general, flu is worse than the common cold. Flu symptoms such as fever, body aches, extreme tiredness, and dry cough are more common and intense. Colds are usually milder than the flu. People with colds are more likely to have a runny or stuffy nose. Colds generally do not result in serious health problems, such as pneumonia, bacterial infections, or hospitalization4,5 (Table 2).
| SYMPTOMS | COLD | FLU |
| onset of disease | protracted | sudden |
| fever | rare | high (3 to 4 days) |
| general aches/pains | slight | common, often severe |
| fatigue/weakness | mild | can last 2 to 3 weeks |
| extreme exhaustion | never | early and prominent |
| stuffy/runny nose | common | sometimes |
| sneezing | usual | sometimes |
| sore throat | common | sometimes |
| chest discomfort | mild/moderate | common, maybe severe |
| cough | hacking | common |
| COMPLICATIONS | sinus congestion | bronchitis and pneumonia |
| can be life-threatening | ||
| PREVENTION | none | annual vaccination |
| healthy habits | ||
| antiviral medicine | ||
| TREATMENT | emporary relief of symptoms | antiviral medicine |
Because colds and flu share many symptoms, it can be difficult (or even impossible) to tell the difference between them based on symptoms alone. Special tests that usually must be done within the first few days of illness can be carried out when needed to determine if a person has the flu.
In addition to the flu and the common cold, other respiratory viruses circulate during the flu season and cause symptoms and illness similar to those seen with a flu infection. One of the most important is the respiratory syncytial virus, which is the most common cause of severe respiratory illness in young children as well as the leading cause of death from respiratory illness in those aged 65 years and older.6
INFLUENZA VIRUSES
A virus first isolated in 1933 causes influenza. There are 3 types of influenza viruses: Type A, Type B, and Type C.
Types A and B have been linked to human illness throughout the world. Type A is more common and is usually associated with the more serious epidemics and pandemics. Type B causes more regional outbreaks. Type C infections result only in mild respiratory illness and are not involved with epidemics.7
The flu virus is an Orthomyxovirus and is usually spherical-shaped. Inside the virus, there are 8 segments of single-stranded RNA, which is the virus’ genetic component. Flu viruses are enveloped and covered with rigid projecting spikes. There are 2 basic types of spikes—hemagglutinin (HA) and neuraminidase (NA). HA molecules allow the flu virus to adhere to host epithelial cells and then to penetrate. Its name comes from the fact that HA can agglutinate RBC in tissue cultures. NA molecules facilitate the release and spread of newly formed viral particles (virions) by preventing them from immediately adhering to host cells and to each other. NA also helps flu viruses penetrate the mucous layer of the pharynx. The result is enhanced viral spread.8,9
Human Type A subtypes are identified through the use of a nomenclature system that includes the geographic site of discovery, a specific laboratory identification number, the year of discovery, and in parentheses the HA and NA present (subtype). An example would be A/Hong Kong/156/97 (H5N1). Naming nonhuman Type A flu viruses also includes the host species—A/Chicken/Hong Kong/G9/97 (H9N2). Types B and C do not have subtypes.7
Influenza A viruses are found in many different animals, including ducks, chickens, pigs, whales, horses, and seals. Influenza B viruses circulate widely only among humans. Flu viruses commonly infect wild aquatic birds, which serve as reservoirs of influenza A viruses. Influenza viruses probably have infected these animals for centuries, yet do not cause serious illness.9
There are 15 different HA types and 9 different types of NA for Type A viruses in wild birds. Only H1, H2, and H3 viruses affect humans. The viruses can jump to other birds, including domestic stocks of chickens, turkeys, and ducks before moving on to humans.7
TRANSMISSION OF INFLUENZA VIRUSES FROM ANIMALS TO HUMANS
Pigs can be infected with swine, human, and avian influenza viruses. Infected pigs often get symptoms similar to humans—cough, fever, and runny noses. Because they are susceptible to viruses from different animal sources, there is the potential that they may be infected with viruses from different species (eg, ducks and humans) at the same time. It is possible for the genes of the viruses to mix (reassort) and create a new virus. The new viruses have most of the genes from the human virus, but can have the HA and/or NA of the avian virus. The new virus could then infect humans, but would possess surface proteins not previously seen in human influenza viruses. While it is unusual to acquire influenza infections directly from animals, sporadic human infections and outbreaks caused by certain avian influenza A viruses have been reported.7
Flu viruses are constantly changing with the emergence of new strains and variants. Each year one or 2 subtypes of Type A may be in circulation with one Type B. HA is the main antigen associated with immunity, with NA playing a more minor role.
Small changes in HA composition (antigenic/genetic drift) happen continually over time. Antigenic drift produces variant Type A viruses that can infect partially immune people. A person infected with a particular flu virus strain develops antibody against that virus. As newer virus strains appear, the antibodies against the older strains no longer recognize the “newer” virus, and reinfection can occur. This is the main reason why people can get the flu more than one time. In most years, one or 2 of the 3 virus strains in the influenza vaccine are updated to keep up with the changes in the circulating flu viruses. So, people who want to be protected from flu need to get a flu shot every year.7 Major abrupt changes in HA and NA (antigenic/genetic shift) produce Type A viruses distinct from those that have been circulating. The result could be a new influenza A subtype and populations that have no immunity. Antigenic shift can occur in wild aquatic birds.7 While antigenic drift occurs all the time, antigenic shift happens only occasionally. Type A viruses undergo both kinds of changes; influenza B viruses undergo relatively slow changes in HA over time.7
SPREAD OF INFLUENZA
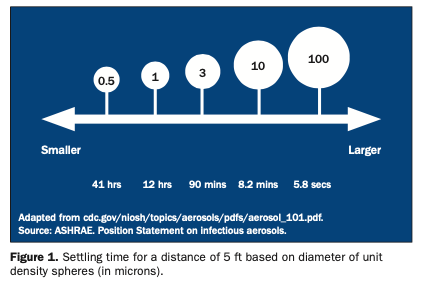
Flu is a contagious disease. The main way influenza is spread is from person-to-person in respiratory droplets associated with coughs and sneezes. This is called droplet spread. This can happen when droplets from a cough or sneeze of an infected person are propelled through the air (usually up to one meter). The droplets are deposited on the nose and mouths of persons nearby. Less frequently, flu viruses are spread when a person touches respiratory droplets on another person or an object and then touches his or her own mouth or nose, or someone else’s mouth or nose before handwashing.2,11
A person can spread the flu starting one day before he or she feels sick. Adults can continue to pass the flu virus to others for another 3 to 7 days after symptoms start. Children can pass the viruses for longer than 7 days. Symptoms start one to 4 days after the virus enters the body. Some persons can be infected with the flu virus but have no symptoms. During this time, those persons can still spread the virus to others.2,4,11
PREVENTING THE FLU
By far, the single best way to prevent the flu is for individuals, especially people at high risk for serious complications from the flu, to get vaccinated each fall (Table 3). Three of the antiviral drugs used to treat influenza have been approved for prevention of influenza. These drugs should not be considered as substitutes for vaccination. All 3 are prescription drugs.12
| Table 3. Target Groups for Annual Vaccination With Influenza Virus Vaccine.5,14 |
|
People at high risk for a complication of influenza: •Persons 50 years old and older •Residents of long-term care facilities •Adults and children with chronic pulmonary or cardiovascular disease, including asthma •Adults and children requiring care for chronic metabolic disease, renal dysfunction, hemoglobinopathy, or immunosuppression, including human immunodeficiency virus infection •Children (6 months to 18 years old) receiving long-term aspirin therapy (a risk factor for Reye’s syndrome) •Women who will be in the second or third trimester of pregnancy during the influenza season (usually December through March)
People who can transmit influenza to those at high risk: •Healthcare personnel •Employees of long-term care facilities •Employees of residences for people at high risk •Providers of home care to people at high risk •Household members, including children of people at high risk
Groups to consider for vaccination: •People at high risk traveling to locations where influenza virus may be circulating •People providing essential community services •Students and others in institutional settings •Any person who wishes to reduce the risk of infection with influenza |
The following groups should not get a flu shot before talking with their physician: people who have a severe allergy to hens’ eggs, people who have had a severe reaction to a flu shot in the past, and people who previously developed Guillain-Barré Syndrome within 6 weeks of having been vaccinated.6
There are 2 types of vaccines that protect against the flu. The “flu shot” is an inactivated vaccine (killed virus) that is injected, usually in the arm. A different kind of vaccine called the nasal-spray flu vaccine (LAIV, live attenuated influenza vaccine) was approved in 2003.
On the basis of antigenic analyses of recently isolated influenza viruses, epidemiologic data, and post-vaccination serologic studies in humans, the Food and Drug Administration recommended that the 2004 to 2005 trivalent influenza vaccine for the United States contain A/New Caledonia/20/99-like (H1N1), A/Fuijian/411/2002-like (H3N2), and B/Shangai/361/2002-like viruses. These viruses were selected be-cause of their growth potential and because they are representative of influenza viruses likely to circulate in the United States during the 2004 to 2005 flu season. These viruses will also be used in the live attenuated influenza vaccine, and all are initially grown in embryonated hen’s eggs. Both vaccines might contain limited amounts of residual egg protein.3,8,9
A single injection of vaccine is needed. When the “match” between vaccine and circulating strains is close, the vaccine prevents influenza in about 70% to 90% of healthy persons under the age of 65 years. Among elderly nursing home residents, the flu shot is most effective in preventing severe illness, secondary complications, and deaths related to the flu. In this population, the shot can be 50% to 60% effective in preventing hospitalization or pneumonia and 80% effective in preventing death from the flu.6
The inactivated vaccine contains no live viruses, so recipients cannot become infected. The risk of a flu shot causing serious harm or death is extremely small. However, a vaccine, like any medicine, may rarely cause serious problems, such as severe allergic reactions. Almost all people who get influenza vaccine have no serious problems with it. The most common side effects, when they occur, include soreness, redness, or swelling where the injection was given, low-grade fever, and aches.3,5,6
The nasal-spray flu vaccine (LAIV) is a new flu vaccine that was licensed in 2003. FluMist is different from the other licensed injectable influenza vaccines because it contains weakened attenuated live influenza virus instead of killed viruses, and is administered by nasal spray instead of by injection.6,10
Attenuated means the viruses are weakened and will not cause severe symptoms often associated with influenza illness. The viruses are temperature-sensitive and cold-adapted. This means that the replication of the viruses is limited at temperatures between 38ºC to 39ºC, which restricts the LAIV viruses from replicating efficiently in human lower airways. Cold-adapted means the viruses replicate efficiently at 25ºC, which is a temperature for replication of LAIV viruses, but restrictive for replication of different wild-type viruses.10,14
LAIV is approved for use in healthy people between the ages of 5 and 49 years. Persons with chronic diseases should not receive LAIV. In clinical studies, transmission of vaccine viruses to close contacts has occurred only rarely. The current estimated risk of getting infected with vaccine virus after close contact with a person vaccinated with the nasal-spray flu vaccine is low (0.6% to 2.4%). Because the viruses are attenuated and cold-adapted, infection is unlikely to result in influenza illness symptoms since the vaccine viruses have not been shown to mutate into typical or naturally occurring influenza viruses.14
Use of inactivated inject-able influenza vaccine is preferred for vaccinating household members, healthcare workers, and others who have close contact with people who have weakened immune systems because of the theoretical risk that a vaccine virus could be transmitted and cause illness. Otherwise, either inactivated vaccine or the nasal-spray flu vaccine can be used for healthy people between the ages of 5 and 49 years who are in close contact with other people at high risk for flu-related complications (eg, people with heart disease who are not on medications that could weaken the immune system).14
TREATING INFLUENZA
How should the flu be treated? Treatment includes rest, drinking plenty of liquids, avoiding the use of alcohol and tobacco, and taking medications to relieve the symptoms of flu. Aspirin should never be given to children and teenagers who have flu-like symptoms—and particularly fever—without first speaking with the patient’s primary healthcare provider.12
In some cases, physicians will choose to use certain antiviral drugs to treat the flu. Antiviral drugs do not cure the flu. Rather, drug treatment, if started within the first 2 days of illness, can reduce the duration of the disease. Four different antiviral drugs (amantadine, rimantadine, zanamivir, and oselt-amivir) have been approved for treating the flu. All 4 drugs will reduce the duration of the flu by a day if taken early. The 4 drugs differ in terms of side effects. The drugs have effect on influenza viruses, but are not effective against bacterial infections that could be complications of influenza.12
The Organization for Safety & Asepsis Procedures (OSAP) is dentistry’s prime source for evidence-based information on infection control and prevention and human safety and health. Information about influenza is available on the OSAP Web site at osap.org.
References
1. Palenik CJ. The flu season. RDH. 2003;23:86-87.
2. Centers for Disease Control and Prevention. Influenza: the disease. Available at: http://www.cdc.gov/flu/about/disease.htm. Accessed: August 2004.
3. Centers for Disease Control and Prevention. Update: influenza activity – United States and worldwide, 2003-04 season, and composition of the 2004-05 influenza vaccine. MMWR Weekly. 2004;53(25):547-552.
5. Centers for Disease Control and Prevention. Prevention and control of influenza: recommendations of the Advisory Committee on Immunization Practices (ACIP) [published correction appears in MMWR Weekly. 2004;53(32):743]. MMWR Recomm Rep. 2004;53(RR-6):1-40.
6. Centers for Disease Control and Prevention. Questions & answers: flu shot. Available at: http://www.cdc.gov/flu/about/qa/flushot.htm. Accessed: August 2004.
7. Centers for Disease Control and Prevention. The influenza (flu) viruses. Available at: http://www.cdc.gov/flu/about/fluviruses.htm. Accessed: August 2004.
8. Centers for Disease Control and Prevention. 2004-05 vaccine. Available at: http://www.cdc.gov/flu/professionals/vaccination/2004.htm. Accessed: August 2004.
9. Centers for Disease Control and Prevention. Inactivated influenza vaccine: what you need to know, 2004-2005. Available at: http://www.cdc.gov/nip/publications/VIS/vis-flu.pdf. Accessed: August 2004.
10. Centers for Disease Control and Prevention. Live, intranasal influenza vaccine: what you need to know, 2004-2005. Available at: http://www.cdc.gov/nip/publications/VIS/vis-flulive.pdf. Accessed: August 2004.
11. Palenik CJ. Flu season, 2003-2004. Dent Economics. 2003;93:118.
12. Centers for Disease Control and Prevention. Questions & answers: preventing the flu. Available at: http://www.cdc.gov/flu/about/qa/preventing.htm. Accessed: August 2004.
13. Couch RB. Prevention and treatment of influenza. N Engl J Med. 2000;343:1778-1786.
14. Centers for Disease Control and Prevention. Live, attenuated influenza vaccine recommendations. Available at: http://www.cdc.gov/flu/professionals/vaccination/live.htm#using. Accessed: August 2004.
Dr. Palenik has held over the last 25 years a number of academic and administrative positions at Indiana University School of Dentistry. These include professor of oral microbiology, director of human health and safety, director of central sterilization services, and chairman of infection control and hazardous materials management committees. Currently he is director of infection control research and services. Dr. Palenik has published 125 articles, more than 290 monographs, 3 books, and 7 book chapters, the majority of which involve infection control and human safety and health. Also, he has provided more than 100 continuing education courses throughout the United States and 8 foreign countries. All questions should be directed to OSAP at office@osap.org.