
EMERGENCY MANAGEMENT
Imagine the following scenario. In the middle of a busy day, a patient presents with a severe toothache or swelling. You may wonder if you could (or should) manage this with a prescription, or if you need to treat this problem invasively and immediately. In nearly all cases, a true emergency of endodontic origin needs to be managed right away. No pain medication and/or antibiotic will truly help.1
This article will review how you should manage an emergency of endodontic origin and, in addition, how to do so efficiently. This will be divided into the following key steps: diagnosis, anesthesia (especially of “hot teeth”), canal instrumentation, and post-op pain and infection management.
DIAGNOSIS
The first and obvious step involves figuring out what is and where is the source of the pain, and if it is tooth-related. Make sure to rule out non-endo related symptoms (ie, periapical inflammation due to parafunction or pain of periodontal origin). Perform all the essential and routine diagnostic endodontic tests (ie, pulp tests, percussion, palpation, biting on a Tooth Slooth). If the emergency is found to be of endodontic origin and you have localized the problem tooth, then proceed with root canal treatment.1
 |
 |
| Figure 1. Periodontal ligament (PDL) injection/intraligamentary injection using a 30-gauge (g) short needle. | Figure 2. PDL injection using a 30-g short needle with rubber dam isolation. |
ANESTHESIA
This is often the most difficult and important aspect of the emergency. Without profound pulpal anesthesia, it is difficult to proceed. Insufficient or lack of anesthesia may turn the appointment into a memorable nightmare for the patient and be very stressful for everyone involved.
Maxillary Teeth
Traditional local infiltration will suffice for most cases in the maxilla. But, make sure to have the needle tip deposit the anesthetic superior to the apices of the involved tooth. For instance, if you are treating a maxillary first molar, try not to hit the zygoma with the needle. This may result in deposit of the anesthetic inferior to the site of innervation to the involved tooth and compromise pulpal anesthesia.
 |
 |
 |
| Figures 3 to 5. (3) Slow-speed Stabident (Fairfax Dental) perforator oriented at base of papilla between teeth. (4) Perforator drilled fully into site. (5) Corresponding short needle fitting into hole prepared by perforator. |
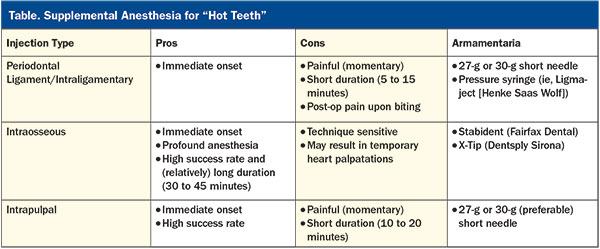
“Hot Teeth”
Arguably, the most difficult tooth to anaesthetize is the infamous “hot tooth,” especially in mandibular posterior teeth. Such cases are well known to remain with feeling in the nerves after more than one carpule of local anesthetic, regardless of the kind of mandibular block technique employed. It has been shown by numerous clinical studies that mandibular blocks will only provide pulpal anesthesia in about one half of the cases presenting with irreversible pulpitis. This is irrespective of the anesthetic type, amount, or time given for onset. So, if your patient presents with acute lingering pain to cold, there’s only about a 50% chance that any mandibular block will suffice.2 This means that in those approximate 50% of cases, you will require supplemental anesthesia (Table). These include the following:
 |
 |
| Figure 6. Stabident slow-speed perforator and corresponding short needle. | Figure 7. X-Tip (Dentsply Sirona) short needle seen fitting into perforator that is drilled into place with a slow-speed handpiece. |
 |
 |
| Figure 8. Macro view of 30-g short needle and syringe used for intrapulpal injection. | Figure 9. Close-up view of needle engaged in canal for intrapulpal injection. |
1. Periodontal Ligament (PDL) Injection, or Intraligamentary Injection—This is performed using a 30-gauge (or possibly 27-g) short needle that is placed at the mesial or distal line angles of the tooth’s periodontal crevice and with the bevel toward the tooth (Figures 1 and 2). Under pressure, a small amount of anesthetic is injected. Onset is quick, but the anesthesia is relatively short-lasting. This injection is often uncomfortable, and patients may complain of the tooth feeling elevated postoperatively. PDL injections may be used as supplemental anesthesia for maxillary and mandibular teeth.3,4
2. Intraosseous—This type of injection has been shown to provide exceptionally high rates of immediate and profound pulpal anesthesia, including in hot teeth. It is used primarily for mandibular posteriors. It requires a pilot hole to be drilled with a special slow-speed instrument (perforator) into the cortical bone between the teeth at the base of the papilla and angled apically. Into the pilot hole, a corresponding short needle is inserted and the anesthetic is slowly deposited (Figures 3 to 5). Its duration is approximately 30 to 45 minutes. However, it is technique sensitive, especially when it comes to carefully drilling the pilot hole and avoiding the roots. Also, it is recommended that an anesthetic with little epinephrine (ie, 1:200,000 epi) be used to minimize heart palpitations.4 The 2 options available are the Stabident (Fairfax Dental) and X-Tip (Dentsply Sirona) (Figures 6 and 7).
3. Intrapulpal—This is oft
en considered the anesthetic of last resort. When performed properly, it is immediate but will only provide about 10 to 20 minutes of profound anesthesia. As with PDL injections, it is very painful in the moment it is administered.5 The needle should engage in the canal, and for this to work, you must obtain resistance/back-pressure when injecting the anesthetic (Figures 8 and 9).
At this point, I suggest pulp testing the tooth prior to the access procedure to make sure it is adequately anaesthetized. There is nothing worse than a nervous emergency patient with a hot tooth jumping from more pain. And, once anesthetized, you must isolate the tooth with rubber dam prior to initiating root canal treatment.
 |
 |
 |
 |
 |
| Figures 10 to 14. (10) Pre-op buccal abscess over tooth No. 14. (11) Buccal incision made with No. 15 scalpel. (12) Purulence draining from incised fluctuant abscess. (13) Curved hemostat used to open incised site. (14) Monoject (Medtronic) syringe used to irrigate inside incision site. |
SOFT-TISSUE ABSCESS OF ENDODONTIC ORIGIN
If your patient presents with a soft-tissue swelling that is fluctuant, you should perform an incision and drainage (Figures 10 to 14). You should use a sharp scalpel and penetrate the “pointing” part of the abscess until you hit bone. A curved hemostat should be used to expand the incision site and help provide a way for the purulence to drain. The site should also be irrigated with a Monoject (Medtronic) syringe. In the case of significant swelling, a drain should be placed. This can be accomplished by using a clean rubber dam cut in the form of the letter T with the top of the letter inserted into the incision site and sutured into place.
ROOT CANAL INSTRUMENTATION
By now you have diagnosed and identified the endo problem, anesthetized the patient, and accessed the tooth. Next comes the canal instrumentation. It may be difficult in the heat of the moment, but do make sure to locate and treat all the canals. This is much easier if magnification with enhanced illumination is incorporated. Dental loupes with a headlight, such as Designs for Vision or SurgiTel, or a dental microscope, such as Carl Zeiss or Global Surgical, are exceptionally helpful, if not priceless. This is especially the case in teeth with artificial crowns or teeth with calcified canals.
If endodontic treatment is not to be completed that day, it is very important to completely instrument each canal. Anything less means leaving behind inflamed or infected pulp tissues. That is why partial pulp extirpation (ie, pulpotomy) is rarely recommended. By definition, a pulpectomy involves complete pulp extirpation and canal instrumentation.1 Furthermore, copious amounts of hypochlorite irrigation should be used, and the canals should be medicated with calcium hydroxide between appointments.
 |
When one is managing an endodontic emergency, it is extremely helpful to utilize an instrumentation system that is simple, efficient, and easy to use. The trend in endodontic instrumentation has been to achieve the same or better clinical and biological outcomes, with fewer steps and instruments. Single-file mechanized NiTi instrumentation is a relatively recent addition to endodontics. Thanks to its simplicity and efficiency, it is well-suited for a variety of tasks, including emergency root canal treatments. An example would be the WaveOne Gold (Dentsply Sirona) reciprocating NiTi file. This file system has been shown to be safer, simpler, and more efficient to use than many rotary NiTi systems6 (Figure 15). With respect to rotary NiTi files, there are newer systems that still require multiple files, but which work more efficiently and require slightly fewer NiTi files than older systems. An example is the ESX series of files (Brasseler USA).
POSTOPERATIVE MANAGEMENT
Occlusion
From a pain management perspective when possible (ie, not on crowned teeth), it is recommended to lighten (lightly reduce) the occlusion of the involved tooth. The intention is to prevent post-op occlusal trauma to the tooth and periapical area that needs to be left alone to settle, so to speak. This is especially important in patients with parafunction habits who may be more likely to traumatize the problem tooth (Figure 16).
 |
 |
| Figure 15. WaveOne Gold (Dentsply Sirona) reciprocating files. Available in 4 sizes. | Figure 16. Occlusal reduction performed with a football-shaped diamond bur. |
Pain Management
As a rule of thumb, if a patient presents with preoperative pain (except for pain to cold and hot), they are likely to experience postoperative pain.7 In turn, you should prepare your patient for this, also providing the individual with analgesics suitable for his or her level of pain. For a healthy patient, these may range from 600 mg of ibuprofen every 6 hours for mild pain to one to 2 Tylenol No. 3 (with codeine) every 4 to 6 hours for more severe pain.
Infection Management
It is very rare that antibiotics will be indicated postoperatively for endodontic emergencies. When the etiology is managed properly endodontically, antibiotics will rarely be need
ed. That is, unless the patient presents with a space infection or systemic symptoms.8 For routine cases and patients, the antibiotic of choice is amoxicillin (500 mg, every 8 hours). For patients with penicillin allergies, clindamycin is recommended (300 mg, every 6 hours). Both antibiotics should be taken for a week.
CLOSING COMMENTS
One of the greatest challenges in clinical dentistry is managing endodontic emergencies. When performed, it should be done efficiently and under profound pulpal anesthesia. To facilitate locating and instrumenting the canals, enhanced magnification and efficient instrumentation systems should be used.
References
- Hargreaves KM, Berman LH. Cohen’s Pathways of the Pulp. 11th ed. St. Louis, MO: Elsevier; 2016: chapter 18, 706.
- Claffey E, Reader A, Nusstein J, et al. Anesthetic efficacy of articaine for inferior alveolar nerve blocks in patients with irreversible pulpitis. J Endod. 2004;30:568-571.
- Hochman M. Supplemental injection techniques. In: Malamed SF. Handbook of Local Anesthesia. 6th ed. St. Louis, MO: Mosby; 2013: chapter 15, 253.
- Moore PA, Cuddy MA, Cooke MR, et al. Periodontal ligament and intraosseous anesthetic injection techniques: alternatives to mandibular nerve blocks. J Am Dent Assoc. 2011;142(suppl 3):13S-18S.
- Lee M, Winkler J, Hartwell G, et al. Current trends in endodontic practice: emergency treatments and technological armamentarium. J Endod. 2009;35:35-39.
- Ahn SY, Kim HC, Kim E. Kinematic effects of nickel-titanium instruments with reciprocating or continuous rotation motion: a systematic review of in vitro studies. J Endod. 2016;42:1009-1017.
- Hargreaves KM, Keiser K. New advances in the management of endodontic pain emergencies. J Calif Dent Assoc. 2004;32:469-473.
- Henry M, Reader A, Beck M. Effect of penicillin on postoperative endodontic pain and swelling in symptomatic necrotic teeth. J Endod. 2001;27:117-123.
Dr. Haas is a certified specialist in endodontics and lectures internationally. He is a Fellow of the Royal College of Dentists of Canada and is on staff at the University of Toronto Faculty of Dentistry and the Hospital for Sick Children. He maintains a full-time private practice limited to endodontics and microsurgery in Toronto. He can be reached at haasendoeducation.com.
Disclosure: Dr. Haas reports no disclosures.
Related Articles

