
Written by: Edward R. Kusek, DDS
Laser Bacterial Reduction (LBR)
The use of dental lasers for the treatment of moderate periodontal disease is extremely controversial. Dental insurance does not cover this procedure, the American Dental Association does not list a code for this treatment, and the American Academy of Periodontology does not accept this as a viable treatment. This may be the first article discussing the benefit of doing laser bacterial reduction (LBR).
LBR in the laser world is used to treat patients with localized periodontal disease showing pocket levels of 5 mm or less, generalized inflammation, bleeding on probing, and tenderness to the gingival tissues. LBR is a single-treatment procedure to reduce the number of bacteria present.
It has been established that bacteria can lead to systemic diseases such as heart attacks, strokes, dementia, adverse pregnancy outcomes, premature deaths, cancer, and diabetes.1
It is proposed that LBR will reduce the number of bacteria present and thus create healthy soft tissues. This article seeks to show that LBR is a viable, noninvasive method of treating moderate periodontal disease that can lead to chronic periodontal disease. It is this author’s opinion that I have seen the positive effects of LBR clinically, but need to show to the clinical world that LBR can change the bacterial flora in a short period of time, which treatment with ultrasonic and hand-scaling cannot achieve.
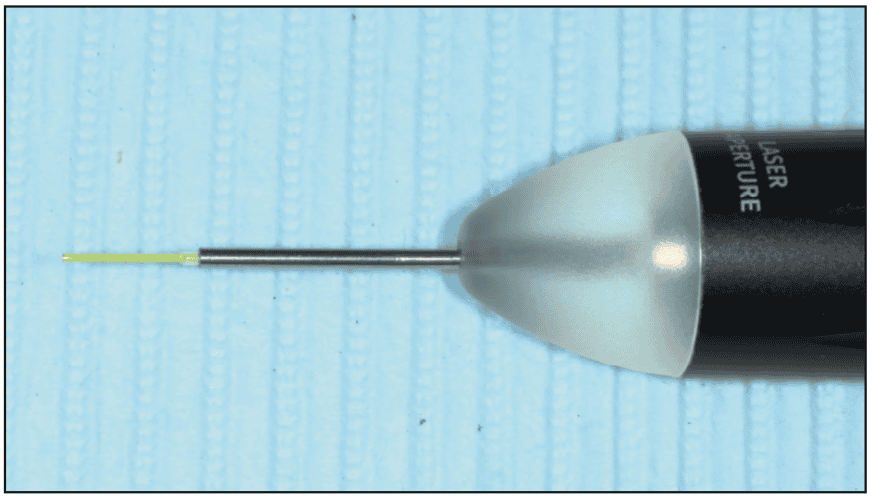
LBR technique uses a noninitiated laser tip (Figure 1), very low energy levels (0.3 to 0.4 W), contact mode, but no tissue interaction. The laser is used in a slow sweeping motion in the gingival pocket, avoiding tissue interaction and treating the circumference of the entire tooth for about 10 to 15 seconds. The goal is to allow laser energy into the gingival tissues to allow heat into the sulcular fluid, thus reducing bacteria in the sulcus. There is no need for topical or local anesthetic as the treatment needs to be done quickly.
My study was accomplished with patients signing a consent to allow the use of scientific data to be distributed for the betterment of dentistry. Patients were chosen to be candidates for the study if they had inflamed tissues on probing, had pockets of no more than 5 mm, and would allow the use of bacterial testing (OralDNA) by taking saliva samples:2
1) after full-mouth probing to determine they would qualify for this study
2) after ultrasonic and hand scaling
3) after full-mouth treatment doing LBR with a diode laser, in this case, the dual-wave Gemini diode laser (Ultradent).
The bacteria that are responsible for periodontal disease and been shown to create aggressive bone loss are: Aggregatibacter actinomycetemcomitans (A.a), Porphyromonas gingivalis (P. gingivalis), Treponema denticola (T. denticola), Tannerella forsythia (T. forsythia) and Fusobacterium nucleatum (F. nucleatum).3 (Note: This author used his own resources to fund this project.)
As noted, the manufactured cleaved tip of the Gemini 810/980 diode was noninitiated. All clinicians, including dental hygienists, were trained in the use of lasers in gingival tissues for both Laser Assisted Periodontal Therapy (LAPT) and LBR, and had certification from the Academy of Laser Dentistry of competence in the use of the diode laser.
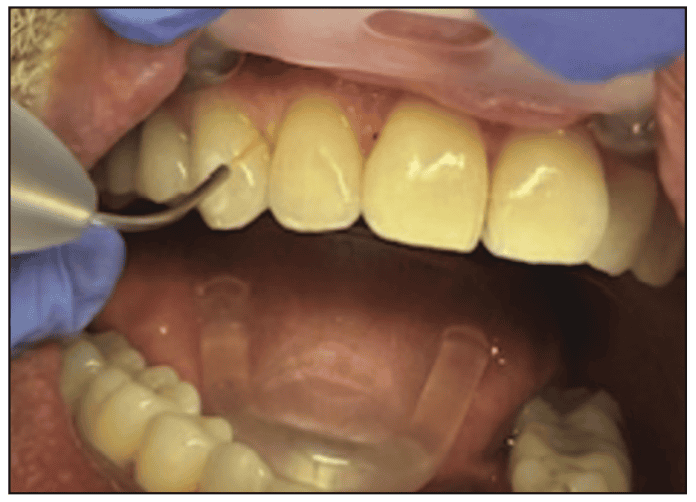
The first step in treatment was to have probing measurements that are current within a month. Treatment would consist of pockets of 5 mm or less. The depth of penetration into the sulcus was to be 1 mm apical to the gingival crest with the tip (Figure 2). Working the tip on the buccal with a swiping motion, moving to the distal and again sweeping the tip 1 mm in depth through the interproximal portion of the tooth, then moving to the mesial portion in the same sweeping motion as described. Proceeding then to the lingual, again sweep 1 mm into the depth of the sulcus. This entire procedure should take no longer than 15 seconds per tooth. This was performed on all teeth that have 5 mm pockets or less that have inflammation, bleeding on probing as described in Figure 2.
RESULTS
Ten out of 12 specimens showed substantial decreases in bacterial counts. The tables (in the online version of this article found at dentistrytoday.com) have shown substantial decreases, except for specimens 2 and 8, which showed increases. After evaluation, the reason for these individuals with increased counts was due to medical issues that created more inflammation (ie, GERD, systemic increase in cholesterol, and decreases in vitamin D). Also this shows that proper training and monitoring with the use of saliva testing to make sure the clinician is using proper technique, that LBR can and does decrease bacteria in the oral cavity.
This study also shows that doing our traditional methods of ultrasonics, scaling and root planing cannot change the bacteria present in the oral cavity. This author was quite surprised, as I was taught that removal of calculus and plaque is the key to reduction in bacteria in the oral cavity.
This study also showed us the importance of saliva testing.4
How can we treat the oral cavity without knowledge of what bacteria we are fighting against? There are several companies that can provide reports of bacteria present in the oral cavity. In addition to OralDNA, there is SimplyPerio and OralPath to name a few.
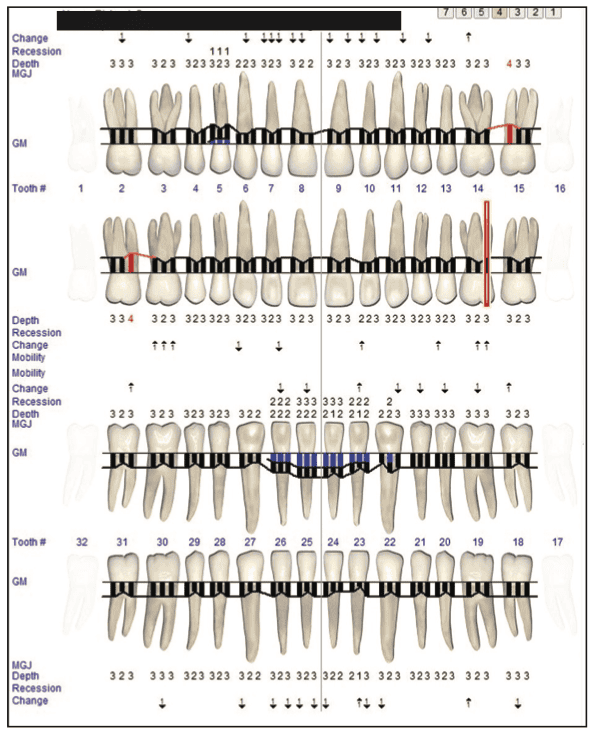
Probing depth on the cases that saw bacterial reduction are shown for 2 of the cases in Figures 3 to 6.



The ADA has provided clinicians with codes that now can be submitted:
- D0417: collection and preparation of saliva sample for laboratory diagnostic testing
- D0418: analysis of saliva sample; Chemical or biological analysis of saliva sample for diagnostic purposes, and
- D0419: assessment of salivary flow by measurement; this procedure is for identification of low salivary flow in patients at risk for hyposalivation and xerostomia, as well as the effectiveness of pharmacological agents used to stimulate saliva production.
We can submit these procedures and codes to insurance companies to help patients, with the understanding that it is up to the actual policy to allow reimbursement for these procedures. As numerous studies have shown, there is certainly a correlation of oral bacteria and systemic issues. In the literature, it is shown that oral bacteria can cause heart disease, stroke, dementia, aneurysm, arterial plaque, pregnancy complications, bone loss, periodontal disease, implant failure, cancer, rheumatoid arthritis, obesity, multiple sclerosis, joint replacement, diabetes, oxidative stress, alterations in immune response and intestinal complications.5-10
Along with the use of LBR, this author has realized the importance of probiotics as another tool to fight oral bacteria.11
CONCLUSION
The online version of this article shares my study results. It is my hope that this article will promote more research on the use of LBR as aid for oral health and systemic health. Dentistry has evolved exponentially since this author started in this profession and I feel that with this and other protocols, our patients will receive the optimum care that they deserve.
REFERENCES
- Monsarrat P, Blaizot A, Kémoun P, et al. Clinical research activity in periodontal medicine: a systematic mapping of trial registers. J Clin Periodontol. 2016;43(5):390-400. doi:10.1111/jcpe.12534
- Johnson AJ, Zhou S, Hoops SL, et al. Saliva testing is accurate for early-stage and presymptomatic COVID-19. Microbiol Spectr. 2021;9(1):e0008621. doi:10.1128/Spectrum.00086-21
- Tonetti MS, Chapple IL, Jepsen S, et al. Primary and secondary prevention of periodontal and peri-implant diseases: Introduction to, and objectives of the 11th European Workshop on Periodontology consensus conference. J Clin Periodontol. 2015;42 Suppl 16:S1-S4. doi:10.1111/jcpe.12382
- Bulfoni M, Sozio E, Marcon B, et al. Validation of a saliva-based test for the molecular diagnosis of SARS-CoV-2 infection. Dis Markers. 2022;2022:6478434. doi:10.1155/2022/6478434
- Jin LJ, Chiu GK, Corbet EF. Are periodontal diseases risk factors for certain systemic disorders–what matters to medical practitioners?. Hong Kong Med J. 2003;9(1):31–7.
- Otomo-Corgel J, Pucher JJ, Rethman MP, et al. State of the science: chronic periodontitis and systemic health. J Evid Based Dent Pract. 2012;12(3 Suppl):20–8. doi:10.1016/S1532-3382(12)70006-4
- Li C, Lv Z, Shi Z, et al. Periodontal therapy for the management of cardiovascular disease in patients with chronic periodontitis. Cochrane Database Syst Rev. 2014;(8):CD009197. doi:10.1002/14651858.CD009197.pub2-
- Beck JD, Papapanou PN, Philips KH, Offenbacher S. Periodontal Medicine: 100 Years of Progress. J Dent Res. 2019;98(10):1053–62. doi:10.1177/0022034519846113
- Slots J. Life-threatening pathogens in severe/progressive periodontitis: Focal infection risk, future periodontal practice, role of the Periodontology 2000. Periodontol 2000. 2020;84(1):215–6. doi:10.1111/prd.12375
- Falcao A, Bullón P. A review of the influence of periodontal treatment in systemic diseases. Periodontol 2000. 2019;79(1):117–28. doi:10.1111/prd.12249
- Seminario-Amez M, López-López J, Estrugo-Devesa A, et al. Probiotics and oral health: A systematic review. Med Oral Patol Oral Cir Bucal. 2017;22(3):e282-e288. doi:10.4317/medoral.21494
ABOUT THE AUTHOR
Dr. Kusek graduated from the University of Nebraska Dental School in 1984. He is a Diplomate of the American Board of Oral Implantology and a Fellow of the American Academy of Implant Dentistry (AAID). He has Mastership in the Academy of Laser Dentistry (ALD) and the AGD. Dr. Kusek is a past president of the ALD, the immediate past president of the AAID, and an adjunct professor for the University of Nebraska Dental School and in the University of South Dakota’s dental hygiene program. He can be reached at [email protected].
Disclosure: Dr. Kusek is a key opinion leader for Ultradent Products and receives some honorarium for lectures.



