


Nickel titanium (NiTi) rotary files have been a key component of endodontic therapy for nearly 30 years. We have seen various files introduced, multiple rotary techniques developed, and enormous marketing efforts promulgated over the decades. In addition to basic concepts such as file design and protocols, we have seen advanced material science and metallurgy introduced as well. Consequently, it is an appropriate time to evaluate some of these advancements. However, before we discuss more specific metallurgy treatments, a basic review of general rotary file design is in order.
BLANK DESIGN
The vast majority of rotary files are ground, not twisted. The majority of commercial rotary files have designs that create significant engagement against the dentinal walls. However, there are a number of files that attempt to reduce this engagement through ingenious blank design. The blank design is very important because it will influence the flexibility of the file and lateral resistance. The move has been away from thick radial lands that rub against canal walls to that of a reamer design (triangular) or something similar (anatomic shaping) without radial lands. This results in greater cutting efficiency.1 Furthermore, after various patents expired on NiTi rotary files, there has been a corresponding increase in the number of rotary systems using various blank designs both globally and in the United States.
METAL TREATMENT
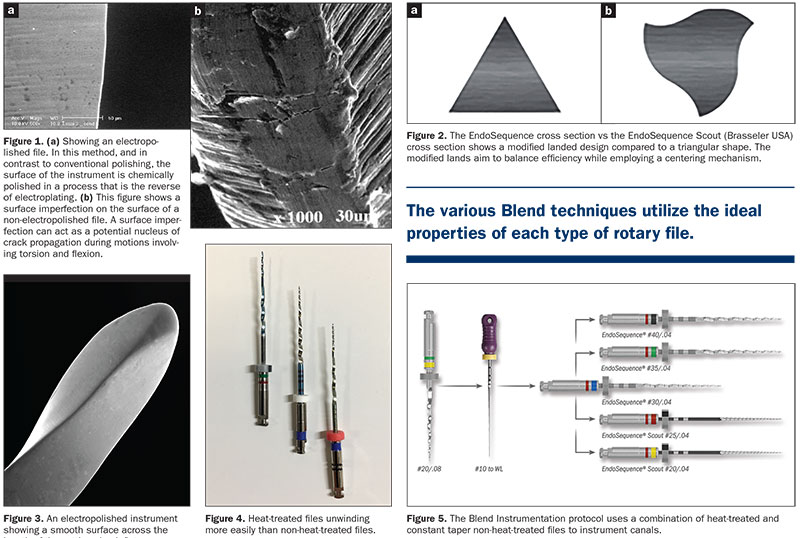
Metal treatment historically has been underutilized in the manufacturing of NiTi rotary files. One of the first heat-treated protocols was the process of electropolishing. Electropolishing will create a very efficient cutting edge as well as reduce the potential for crack propagation (Figure 1). Additionally, dental manufacturers discovered that heat treating NiTi wire generates numerous benefits in the performance of a file.2 The 2 most significant changes are increased flexibility and greater resistance to cyclic fatigue.2
 |
QUALITY OF MANUFACTURING
Although many clinicians may not completely understand the ability to evaluate a NiTi blank’s quality, it is nonetheless important. Quality can be seen in a blank’s flexibility and shape memory. Quality of manufacturing can also be seen if the handle of the file detaches during engagement. Another good test of an instrument’s quality is turning the file around and looking straight down on the file as it rotates in the handpiece. Is the file running in a true repeatable pattern, or are there discrepancies? In order to attain precision and predictability in our endodontics, we need to employ quality instruments. Ultimately, this is a decision left to the clinician.
ENDOSEQUENCE BLANK DESIGN
The original EndoSequence file’s blank design was considered revolutionary when introduced and remains a very successful innovation. It has been designed so that there are alternate contact points along the shank of the instrument. This innovative design keeps the file centered in the canal, and the alternating contact points (ACPs) also reduce the torque requirements of the file. This is because the ACPs reduce the lateral resistance of the file. However, EndoSequence (Brasseler USA) now has a new addition to its line (EndoSequence Scouts [Brasseler USA]), and these files employ a different blank design (Figure 2).3
The EndoSequence Scouts employ an “old school” rotary file design from the 1990s that actually utilizes a small radial land. While this design was acceptable as a non-heat-treated file, it turns out to be an incredible design when using heat-treated wire.
The EndoSequence Scout files come in only 6 sizes: 15, 17, 20, 25, 30, and 35. The size limitation is such because these instruments act like canal negotiators, meaning that they are creating a glidepath down curved and tortuous canals. Because this type of activity demands utmost centering of the file, the EndoSequence Scouts, as a result of their small radial land, stay centered in the most demanding of canals. The reduced length of the cutting shank on the Scouts (12 mm) is because they are indicated as scouting instruments, not full shank rotary files.
ENDOSEQUENCE METAL TREATMENT
The EndoSequence file is an instrument that continues to employ electropolishing. However, the new EndoSequence Scout files, which have a different blank design (the incorporation of a very small radial land), are not electropolished. Instead, these files, which have been specifically designed for “scouting” purposes, have been heat-treated (Figure 3).4
As previously mentioned, one of the more recent advancements in clinical endodontics has been the introduction of heat-treated NiTi files. The specific temperature that the files are exposed to can vary from manufacturer to manufacturer, but there are a few constants. Heat-treated rotary files exhibit some very positive characteristics, and a quick discussion of temperature-induced phase change in NiTi is in order.
At room temperature, NiTi assumes an austenite phase of its molecules. However, when heated, the molecules change their order, and this deformation is referred to as a martensitic transformation. After their change, the wire now assumes a martensite (or goes into a martensitic) phase. But there are some very significant differences associated with this martensitic phase.
Not only are heat-treated files (martensitic phase) much more flexible than non-heat-treated instruments (austenite phase) but, more importantly, they are also exponentially more resistant to cyclic fatigue. This is especially important because excessive cyclic fatigue is a major cause of instrument separation. The accumulation of cyclic fatigue is a far greater concern than excessive torque forces, and this is why instrument developers try to find predictable ways to reduce cyclic fatigue.5
While there are some noteworthy characteristics associated with heat-treated files, they also have some serious limitations. Heat-treated files routinely have their edges roll over during manufacture, and consequently, they are not as effective in cutting and shaping as non-heat-treated (austenitic) files. Furthermore, heat-treated files distort easily and have a nasty tendency to elongate (Figure 4). Therefore, after using a heat-treated #30/.04 rotary file previously measured to a final working length of 21 mm, it may now have become a #28.5/.04 with a length of 22 mm. As a result of the distortion, you will not be able to achieve true endodontic synchronicity if you wish to use a matching gutta-percha cone.
Although the tendency to distort is unfortunate, it does not make heat-treated files any less important. They are stellar when they are employed as scouting instruments negotiating their way down tortuous canals. But to have the final canal shape match a master gutta-percha cone, the canal needs to be “finished” by a non-heat-treated (austenitic) file that will not distort.
The above-listed limitations and benefits of heat-treated instruments inspired Real World Endo to develop a “Blend Technique” wherein one is using a combination of both heat-treated and non-heat-treated files. The goal with the Blend Technique is to employ the respective files where they are most indicated for use. Heat-treated files were initially promoted as helping the clinician get into the orifice at the top of the canal. This was obviously created by sales and marketing people because having difficulty getting into a canal orifice is not a metallurgy issue; it’s an access problem. However, where heat-treated files have an opportunity to display their best characteristics is at the exact opposite end of the canal: the apical third, where the most contentious curvatures are located. Accordingly, the instruments in the Blend Technique are used where they perform best and most efficiently. For example, in straight canals, use a non-heat-treated file (austenitic phase), which cuts better, and in curved canals, use the heat-treated rotary files (martensitic phase) to better navigate the curvatures and to create a glidepath. The preparation created by the heat-treated file is ultimately completed by using a non-heat-treated file, which “finalizes” the preparation.
 |
When creating this technique, it quickly became apparent that austenitic files should be used in the upper coronal two thirds of the canal, and the more flexible heat-treated files (martensitic) should be used in the apical third. This makes so much sense and is completely intuitive. However, the combination of austenitic and martensitic files left us with one more challenge: the conefit!
Real World Endo was the creator of the concept “Precision-Based Endodontics,” along with the ability to create “endodontic synchronicity.”6 Endodontic synchronicity means creating a shape that can be predictably matched by laser-verified paper points, master gutta-percha cones, and even prefabricated posts. This can only occur repeatedly if the final shape is a constant taper.6
To modify the shape created by a combination of austenitic and martensitic files, all we have to do is use one final austenitic file to act as a “finalizing instrument,” and this will blend both preparations together to create a final constant taper preparation. This is what we did for years when we hybridized tapers. Create endodontic synchronicity; obturation then becomes straightforward.
RHYTHM TECHNIQUE
In addition to blank design, the most meaningful way to minimize the accumulation of cyclic fatigue and its associated rate of file separation is to employ the proper technique, which for all EndoSequence files is the rhythm technique.
This technique will actually work well for many different file systems. The rhythm technique is a series of 3 engagements with a rotary file within a root canal, each time advancing farther down the canal until minimal engagement is encountered: One, back-2, back-3, out. The backstroke is only 1 to 1.5 mm as this has been developed to simply disengage the file from the canal wall. Ideally, the operator does 2 cycles of 3 engagements with this technique and then moves on to the next instruments. Additionally, there is a series of tenets associated with the rhythm technique:
1. Always keep the file moving. By doing such, you can maintain control over the file and the procedure. Simultaneously, it disperses the accumulation of cyclic fatigue. When working with rotary files, the worst thing possible is to take a file around a curve and let it stay in one place while rotating. It is easy to think that the file will eventually auger its way down the canal by doing such. This does not happen, and it will actually lead to cyclic fatigue and, ultimately, file separation.
2. Don’t be in the canal longer than 2 to 2.5 seconds. In our Real World Endo courses, we find that dentists have a tendency to stay too long in the canal with their files. Ideally, you should be in the canal for no more than 2 seconds, although certain large canals can extend that. The reason for this is that when working with any rotary file, once the chip space becomes full, the file is no longer working efficiently. Instead, all it is now doing is generating cyclic fatigue as a result of its inefficiency. The only way to clean the chip space is to remove the instrument from the canal and clean it.
3. Never force a file. Let the file do the work by simply advancing it to the next point of engagement. Never lean on the instrument or force it in any manner in an attempt to take it to a preconceived length.7
ENDOSEQUENCE BASIC BLEND TECHNIQUE
The first instrument used when doing a root canal is a #10 stainless steel hand file. This will locate the canal orifice, and then only take it down a few millimeters into the canal space, establishing coronal patency because canals calcify from top to bottom. If a canal is open in the coronal third, it should be a patent canal.
The next instrument is a #20/.08 orifice opener (or something similar), and it is taken down into the canal no more than halfway. Following the opening of the coronal half of the canal, again use a #10 or #15 stainless steel hand file in combination with an apex locator to determine the final working length.
Following the insertion of the orifice opener, the next rotary file is a regular #30/.04 taper EndoSequence file (non-heat treated). Use this file with a rhythm technique and simply employ 2 series of 3 engagements with the instrument. This file is working like a “triage instrument,” meaning that it is acting as a gauging tool. If the 30/.04 reaches the final working length easily, simply do an apical enlargement preparation, which means use 1 or 2 larger files. The size of the specific file is the clinician’s choice. But the best part of the “Blend Technique” is when the triage file (#30/.04 EndoSequence file) comes up short of the final working length. Now switch over to a crown-down technique, and also switch to the heat-treated files (EndoSequence Scouts), which, as noted, have been specifically designed to work better in curvatures (Figure 5).
Begin with the #25 Scout, and after 2 passes with the rhythm technique, if you are still short of the final working length, step down to the #20. In most cases, including molars, the #20 Scout will get you to the final working length. But are we finished? No, because we do not have endodontic synchronicity; everything does not match due to the distortion associated with heat-treated instruments. The ideal way to restore synchronicity is simple. Just take the original triage file (#30/.04 EndoSequence file) all the way to length. You will be surprised how easily this austenitic file goes down the canal, and now you have blended both the austenitic and martensitic preparations into one final constant tapered shape (Figures 6 to 8).
ENDOSEQUENCE ADVANCED BLEND TECHNIQUE
The Advanced Blend Technique has been designed for practicing endodontists, as this group is generally treating the most difficult cases (think very narrow, curved canals). In order to modify the original Blend Technique for our fellow endodontists, we made a few simple changes.
The opening of the coronal half of the canal, as well as the establishment of the final working length, is the same. However, it is in the use of the triage file where the protocol differs. With the basic technique, a #30/.04 regular (non-heat-treated) EndoSequence file is used as the triage instrument. However, with the advanced technique, due to the more difficult cases being treated, a #25/.04 EndoSequence file (non-heat-treated) is substituted as the triage instrument. Subsequently, if the #25/.04 comes up short of the working length, you can slide over to the heat-treated Scout files, beginning with a size 20. Work that with 2 series of 3 engagements (rhythm technique), and if it continues to be short, proceed to work the #17 Scout in a crown-down fashion. If the canal is so gnarly that the #17 doesn’t reach final working length, continue the crown-down with the #15 Scout, which will get you to the final working length. Following the application of the Scout files, the preparation is completed (finished) by using the original #25/.04 triage file. Indeed, if desired, one can increase that size to a #30/.04. With either size, the master cone will now fit in a precise manner (Figure 9).
ENDOSEQUENCE .06 TAPER BLEND TECHNIQUE
A third Blend technique, and one that is gaining in popularity, is the use of .06 tapers! Real World Endo introduced EndoSequence .06 tapers in 2003 with the difference being that they stopped the range of sizes at size 50. In fact, during presentations, it was recommended not to use .06 tapers in any size larger than a size 40. However, as we have gained greater knowledge in our understanding of rotary file instrumentation, we realized that there is indeed a place for .06 tapers and the numerous advantages associated with such a technique. The advantages are:
1. You can still do conservative preparations with .06 tapers. The key is using nothing larger than a #30/.06 taper. In fact, the .06 tapers that are recommended with the new Blend technique correspond to the “small” packages associated with the original EndoSequence technique. The sizes are 15, 20, 25, and 30/.06 taper.
2. The use of .06 tapers make the use of heated gutta-percha techniques easier to perform predictably. If one uses a warm vertical condensation technique or a carrier-based approach, both are much easier to perform with a .06 taper preparation.
3. Improved irrigation capability. Studies have shown that a #30/.04 taper preparation is more than adequate to handle all of our irrigation demands. However, with the recognition of enhanced irrigation techniques activated by the use of ultrasonics, it is far easier to generate effective acoustic streaming and 3D cleaning (webs, fins, canal anastomoses) with a .06 taper preparation.
4. Primary conefit. Even for those dentists employing a sealer-based approach to obturation (EndoSequence BC Sealer [Brasseler USA]), the primary conefit is considerably easier with a .06 taper preparation (Figure 10).8
IN SUMMARY
The various Blend techniques utilize the ideal properties of each type of rotary file. The key is to finish with one non-heat-treated file, thereby ensuring that synchronicity is established and that the master cone fits properly. This technique has become very popular with endodontists because they realize that it is totally intuitive. It will also save you time during the overall procedure and will be conservative in the coronal third of the root.
References
- Koch KA, Brave DG. Real world endo: Design features of rotary files and how they affect clinical performance. Oral Health. February 2002:39-49.
- Anderson ME, Price JW, Parashos P. Fracture resistance of electropolished rotary nickel-titanium endodontic instruments. J Endod. 2007;33(10):1212–6. doi:10.1016/j.joen.2007.07.007
- Koch KA, Brave DG. The EndoSequence file: A guide to clinical use. Compend Contin Educ Dent. 2004;25(10A):811–3.
- Schäfer E, Oitzinger M. Cutting efficiency of five different types of rotary nickel-titanium instruments. J Endod. 2008;34(2):198-200. doi:10.1016/j.joen.2007.10.009.
- Zupanc J, Vahdat-Pajouh N, Schäfer E. New thermomechanically treated NiTi alloys – a review. Int Endod J. 2018;51(10):1088-1103. doi:10.1111/iej.12924
- Koch KA, Brave DG. EndoSequence: Melding endodontics with restorative dentistry, part 3. Dent Today. March 2009:88-95. https://www.dentistrytoday.com/endodontics/1005–sp-319519306.
- Koch KA, Brave DG. Real world endo sequence file. Dent Clin North Am. 2004;48(1):159–82. doi:10.1016/j.cden.2003.11.004
- Koch KA, Brave DG. The 0.06 tapered preparation “secret technique” of endodontists. Dent Today. September 2002:68-74.
Dr. Koch received both her DMD degree and certificate in endodontics from the University of Pennsylvania School of Dental Medicine (Penn Dental). She is also the founder and past director of the Postdoctoral Program in Endodontics and Microsurgery at the Harvard School of Dental Medicine. Following her clinical and academic career, she formed her own successful technology and development company, Real World Endo, of which she was CEO and President. Dr. Koch is the holder of multiple patents, maintains a faculty position in the Department of Endodontics at Penn Dental, and serves as a Senior Fellow with Penn Medicine. She is also a member of the Board of Overseers for Penn Dental and maintains an adjunct faculty position at the Harvard School of Dental Medicine. She can be reached at annelaurenkoch@gmail.com.
Dr. Nasseh received his Master of Medical Science degree and certificate in endodontics from the Harvard School of Dental Medicine in 1997. He received his DDS degree in 1994 from Northwestern University Dental School. He maintains a private endodontic practice in Boston (msendo.com) and holds a staff position in Harvard’s postdoctoral endodontic program. Dr. Nasseh has lectured extensively on such diverse topics as diagnosis, anesthesia and sedation, and microsurgery. He is the endodontic editor for several dental journals and periodicals and is on the clinical advisory board of the Michigan-Pittsburgh-Wyss Center for Regenerative Medicine. He is the CEO and president of Real World Endo (realworldendo.com). He can be reached at anasseh@hsdm.harvard.edu.
Disclosure: The authors are shareholders in Real World Endo and serve as consultants for Brasseler USA.
Related Articles
What’s Going on in Dental Schools?
Preventive Endodontics: The Art of Avoiding a Root Canal
Dr. Marty Jablow and Handpiece Versatility








