
Written by: Drs. Casey Bennett & Gregori Kurtzman
INTRODUCTION
Three-dimensional printing continues to improve clinical timelines while expanding predictable in-house lab fabrication of prosthetics. Regarding removable prosthetics, flexible partial dentures have traditionally required outsourcing to a lab and injection-molding workflows that limit efficiency. The introduction of SprintRay’s Apex Flex partial base resin represents a significant step forward, enabling clinicians and laboratories to fabricate flexible partial denture bases chairside or at a laboratory.
Apex Flex is a biocompatible material with FDA Class II (510[k]) clearance that is engineered specifically for additive manufacturing of flexible partial denture bases. The material is designed for use with the Pro 2 3D printer (SprintRay) and the NanoCure post-curing system (SprintRay). Apex Flex allows practices to transition flexible partial production from an outsourced laboratory to a controlled, predictable in-house process. The resin material is available in 2 gingival shades—standard pink and light pink—providing clinicians with an aesthetic latitude to match a wide range of patients’ gingival shades without the need for secondary characterization.
From a clinical perspective, the base resin achieves a balance between flexibility, strength, and durability that has been difficult to achieve with flexible materials. The material has a flexural strength of ≥26.5 MPa, providing sufficient resistance for clasp engagement and function under masticatory loading. With an elongation until breakage approaching ≥50% this allows the denture base and clasp arms to flex without permanent deformation or fracture. A flexural modulus in the range of ≥700 MPa maintains structural support while preserving patient comfort. Additionally, a work of fracture value exceeding ≥5,000 J/m2 reflects its high resistance to crack propagation that is an important consideration for long-term clinical use by the patient. This translates clinically into a partial denture base that adapts to functional movement, reduces pressure points, and maintains retention without the rigidity associated with conventional acrylic frameworks.
A key strength of Apex Flex lies in its seamless integration into SprintRay’s validated digital workflow. Following intraoral or model scanning, partial denture design is completed in exocad (exocad America), which incorporates templates and design logic optimized for flexible materials. Design can also be done using SprintRay Cloud Design, when the practice does not wish to design the prosthesis themselves. Printing is performed on the SprintRay Pro 2 using manufacturer-validated parameters. This is followed by washing and post-curing in the NanoCure unit to ensure consistent polymerization and material performance. For cases requiring printed denture teeth, Apex Flex can be paired with SprintRay Apex Teeth resin, enabling the fabrication of a complete flexible partial prosthesis entirely within the same digital workflow.
Clinical Advantages
The ability to fabricate flexible partial dentures in-office offers several tangible benefits. Turnaround time can be reduced dramatically, often enabling same-day delivery while eliminating the need for injection-molding equipment or reliance on external laboratories. Keeping production internal enhances cost control and practice profitability. While the digital design process supports repeatability, it reduces the number of adjustment appointments typically associated with traditionally fabricated flexible partials. From a patient perspective, the soft, tissue-friendly feel of Apex Flex improves comfort, particularly for patients who have struggled with rigid acrylic frameworks.
When designing flexible partials, clinicians should be mindful of clasp geometry and support zones. Retention needs to be maximized without over-flexing clasp arms, particularly in distal-extension situations where excessive flexibility may influence denture stability. Proper design planning remains essential to fully leverage the material’s mechanical advantages while preserving soft-tissue comfort. Apex Flex is best suited for tooth-borne partial dentures, particularly in the aesthetic zone where metal clasps are undesirable. As with all flexible materials, caution is advised in long distal-extension cases, in patients with parafunctional habits, or when the inter-arch space is insufficient to allow proper engagement of the flexible clasp without over-thinning the material.
Workflow
Intraoral scanning of the maxilla or mandible should emphasize complete vestibular extension and capture of natural undercuts, which are essential to retention of the flexible prostheses. An opposing arch scan and bite registration are also required. Over-smoothing tissue scans should be avoided, as loss of undercut detail directly compromises partial denture retention. The scan files are exported to exocad when the design will be done in-house or to the SprintRay Cloud Design.
The flexible partial denture template allows controlled definition of saddle thickness (typically 1.5 to 2.0 mm), with strategic designation of flexible clasp zones and relief over frena and in areas of movable mucosa. Tooth replacement may be designed for monolithic printing using Apex Teeth or OnX Tough 2 (SprintRay). Rounded internal transitions are preferred throughout the design to reduce stress concentration and enhance long-term flexural durability.
The design files are exported back to the dental practice, where Apex Flex is printed on the Pro 2 3D printer. The tissue surface is oriented approximately 20º to 30º on the build plate to optimize surface accuracy while minimizing support contact in non-critical areas. Layer thickness should strictly follow the manufacturer’s instructions for use, typically 100 µm. Gentle agitation of the resin bottle prior to printing ensures homogeneity and consistent mechanical performance.
Immediately following printing, the appliance undergoes a primary wash in high-concentration isopropyl alcohol, followed by a secondary rinse in fresh solvent. Excessive washing should be avoided, as prolonged solvent exposure can adversely affect the resin’s elasticity. After complete air drying, post-curing is performed in the NanoCure unit according to the Apex Flex IFU, ensuring full polymerization without residual tackiness. Proper curing is essential to achieving final flexibility, tear resistance, and long-term durability.
The supports are removed with fine diamonds in a high-speed handpiece, and margins are refined using rubber polishers or light pumice at low speed to avoid heat buildup. When teeth are not printed monolithically, printed or prefabricated denture teeth are bonded using SprintRay-approved protocols, with care taken not to alter clasp zones on the intaglio surface.
At delivery, the partial denture is seated passively without force, and retention, aesthetics, and comfort are evaluated. Adjustments should be conservative, limited to polishing rather than grinding flexible clasp areas. Patients are instructed to remove the appliance using bilateral pressure, avoid exposure to hot water, and clean the prosthesis with non-abrasive cleansers.
When properly implemented, this digital workflow allows the clinician to deliver flexible partial dentures the same day.
Case 1: Maxillary Arch
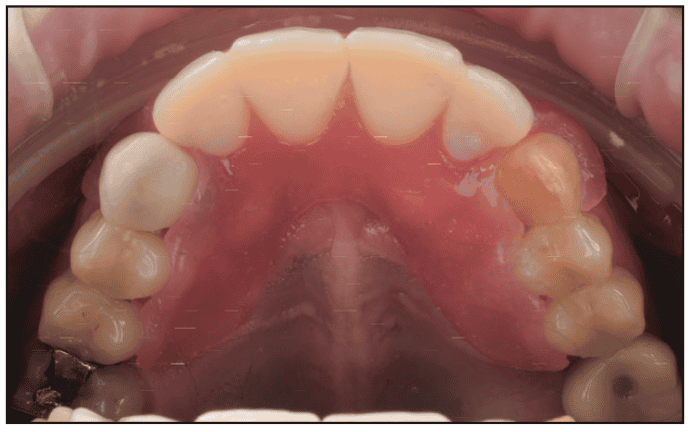
A 41-year-old male patient presented, indicating he had lost his maxillary Valplast partial denture, and requested a new denture. He asked how long it would take to have the new denture made, as he was embarrassed about not having any upper front teeth. Examination noted the only dentition missing on the maxillary arch were the lateral and central incisors bilaterally (Figure 1). The left canine (tooth No. 11) was very badly stained and darker than the right canine (tooth No. 6, which had an old PFM crown shade A2). The patient preferred to match the old A2 PFM crown and did not want to correct the darker canine No. 11 at this time. The patient was informed that a flexible 3D-printed partial denture could be fabricated and delivered that day, and he accepted treatment.

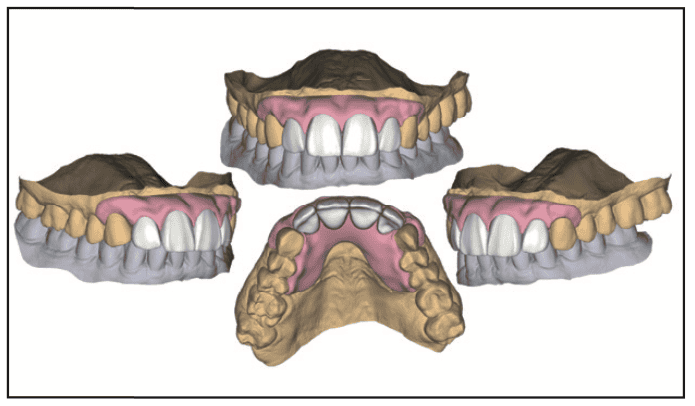
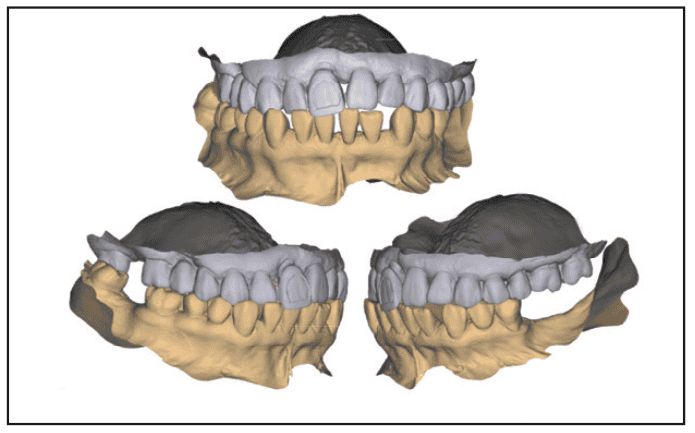
An intraoral scan of both full arches, with the teeth occluded, was performed with a TRIOS 5 scanner (3Shape) and imported into exocad (Figure 2). A shade of A2 was selected to match the PFM crown on the right canine (tooth No. 6). The virtual models were articulated in the software as part of the design phase (Figure 3). The partial was then designed to fit the space with flexible clasps to the existing dentition (Figures 4 and 5). In the software, the virtual denture base (Figure 6) and virtual denture teeth (Figure 7) were separated into separate files, then imported into the SprintRay Print Setup cloud-based nesting software to set up for printing. Supports were added to the virtual denture base and the virtual denture teeth and placed on the virtual platform for printing (Figure 8). The 3D printing of the denture was accomplished with Apex Flex resin in shade standard pink, and the teeth were printed in Apex Teeth shade A2. Upon completion of printing on the Pro 2 printer the denture base and teeth were removed from their individual platforms with supports intact (Figure 9). The supports on the printed teeth were removed with a high-speed handpiece, and they were then luted into the denture base with additional Apex Flex resin, and the Apex Flex workflow was followed as previously outlined to complete the flexible denture (Figure 10). The fabrication process, from capturing the intraoral scans to having the completed partial denture ready for intraoral insertion, took about 2 hours.








The patient was reseated in the operatory, and the flexible partial was inserted (Figures 11 and 12). Fit and retention were verified, and the patient was given a mirror to assess the aesthetic result. He indicated he was happy with the aesthetics (Figure 13).


Case 2: Mandibular arch
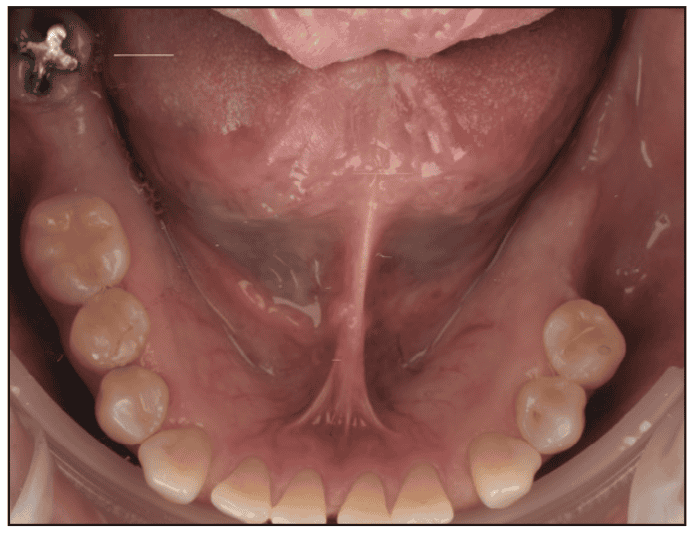
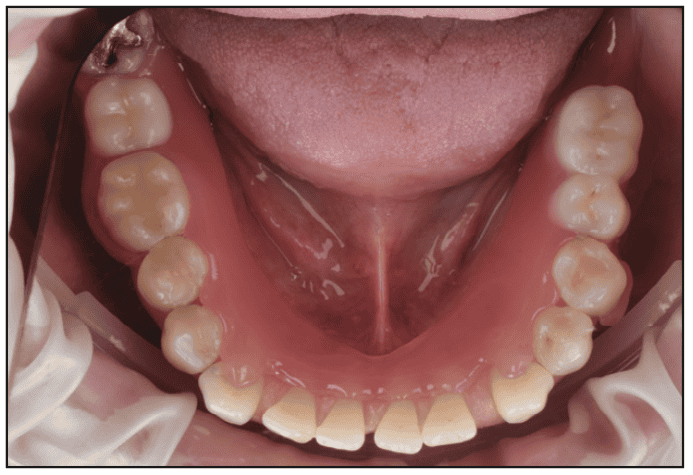
A 66-year-old female patient presented, reporting that she had misplaced her lower partial denture and requested replacement (Figure 14). An intraoral scan of both full arches and the teeth occluded was performed with a TRIOS 5 scanner. A shade of A2 was selected. The patient was dismissed and appointed for insertion of the partial denture a week later.
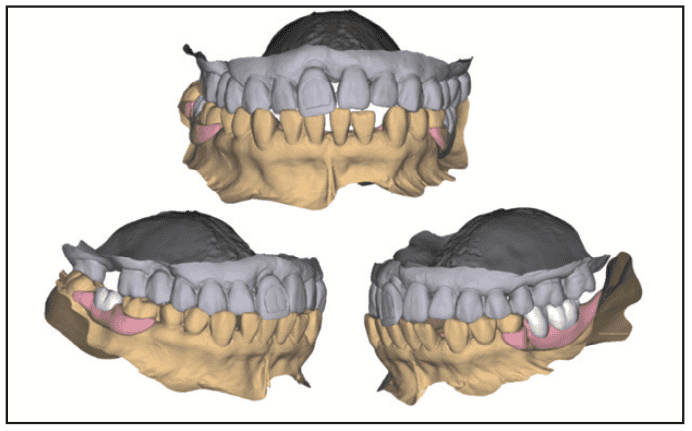
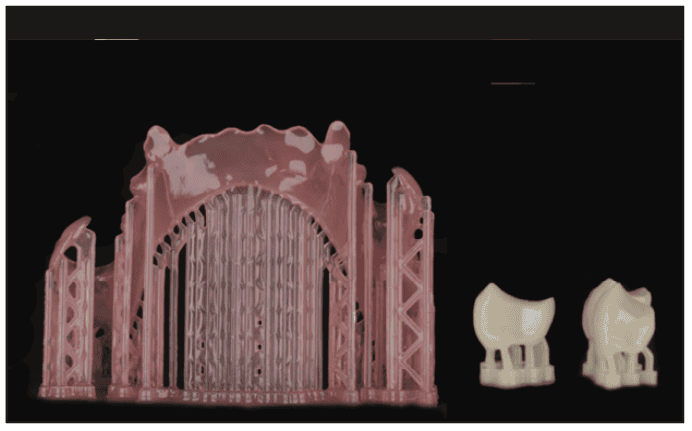
The scan files were imported into exocad (Figure 15). The virtual models were articulated in the software as part of the design phase (Figure 16). The partial was then designed to fit the space with flexible clasps to the existing dentition (Figures 17 and 18). In the software, the virtual denture base and virtual denture teeth were separated into separate files, then imported into the SprintRay Print Setup cloud-based nesting software to set up for printing. Supports were added to the virtual denture base and the virtual denture teeth and placed on the virtual platform for printing. The 3D printing of the denture was accomplished with Apex Flex resin in shade standard pink and the teeth were printed in Apex Teeth shade A2. Upon completion of printing on the Pro 2 printer, the denture base and teeth were removed from their individual platforms with supports intact (Figure 19). The supports on the teeth were removed, and then the teeth were luted into the denture base with additional Apex Flex resin. The Apex Flex workflow, as previously outlined, was followed to complete the flexible denture (Figure 20).



The patient presented a week later and was seated in the operatory, and the flexible partial was inserted (Figure 21). Fit and retention were verified, and the patient indicated she was happy with the fit, retention, and bite.
DISCUSSION
The evolution of digital removable prosthodontics has lagged behind fixed and implant workflows, largely due to material limitations and the complexity of fabricating removable prosthetics. Flexible partial dentures, while well accepted by patients for comfort and aesthetics, have traditionally required injection-molded thermoplastic materials and outsourcing to a laboratory for fabrication. This workflow creates delays, increases cost, and limits the clinician’s ability to control fit, design, and material performance. The introduction of Apex Flex resin within the SprintRay ecosystem represents a meaningful shift in this paradigm.
From a clinical standpoint, the mechanical profile of Apex Flex addresses many of the shortcomings previously associated with printable flexible materials. The combination of moderate flexural strength with high elongation at break allows clasp arms to engage undercuts without inducing localized stress concentrations that can lead to fracture or patient discomfort. Equally important, the elevated work of fracture suggests improved resistance to crack initiation and propagation, an area of concern for flexible partials subjected to repeated insertion-removal cycles and functional loading.
Digitally designed flexible partials also introduce a higher level of consistency compared with analog techniques. Injection-molded appliances are highly technique-sensitive, with outcomes influenced by flasking, processing temperature, and cooling dynamics. In contrast, a validated additive workflow standardizes layer thickness, curing protocols, and material handling. This translates into a more predictable intraoral fit and reduced post-delivery adjustment time. For practices already using in-office 3D printing, Apex Flex extends the return on investment by expanding the range of removable appliances that can be produced internally.
Nevertheless, appropriate case selection and prosthetic design remain critical. While the material exhibits favorable flexibility, excessive reliance on flex for retention, particularly in distal-extension cases, may compromise long-term stability if support zones are inadequately designed. Digital partial frameworks must still respect established removable prosthodontic principles, including strategic support, controlled clasp flexure, and tissue adaptation. Apex Flex does not replace sound design fundamentals; rather, it enhances them.
In the broader context of digital dentistry, Apex Flex highlights an important trend: the migration of traditionally outsourced removable prosthetics into the in-office clinical setting. For clinicians focused on efficiency, patient experience, and practice control, the ability to scan, design, print, and deliver a flexible partial denture, often within a single visit, represents a substantial clinical and operational advantage.
CONCLUSION
SprintRay’s Apex Flex partial base resin expands the practical scope of in-office additive manufacturing by bringing flexible partial dentures into a fully digital, same-day workflow. By combining clinically relevant mechanical properties with a validated printing and post-processing ecosystem, Apex Flex enables clinicians to deliver comfortable, aesthetically pleasing, flexible partial dentures with greater efficiency and control. As digital removable prosthodontics continues to evolve, materials such as Apex Flex position practices to meet patient expectations while maintaining predictability, profitability, and clinical confidence. Flexible partial dentures fabricated additively are likely to become a routine component of the modern in-office prosthodontic armamentarium.
ABOUT THE AUTHORS
Dr. Bennett is a restorative dentist in Charleston, SC, delivering minimally invasive care with in-house digital design and fabrication. He teaches digital restorative workflows to dentists around the world and serves as faculty at the MOD Institute. He can be reached at [email protected].
Dr. Kurtzman is in private general dental practice in Silver Spring, Md, and a former assistant clinical professor at the University of Maryland in the department of Restorative Dentistry and Endodontics and a former AAID Implant Maxi-Course assistant program director at Howard University College of Dentistry. He has lectured internationally on the topics of restorative dentistry, endodontics, implant surgery and prosthetics, removable and fixed prosthetics, periodontics, and has published more than 930 articles globally, several ebooks, and textbook chapters. Dr. Kurtzman has been honored to be included in the “Leaders in Continuing Education” by Dentistry Today annually since 2006 and was featured on their April 2024 cover. He can be reached at [email protected].
Disclosures: Dr. Kurtzman received compensation from SprintRay for writing this article. Dr. Bennett reports no disclosures.


