


Filling root canal systems represents the culmination of a series of procedural steps that comprise start-to-finish endodontics. Root-appropriate shaping promotes 3-D disinfection by removing restrictive dentin, allowing for a more effective volume of irrigant to penetrate, circulate, and potentially clean into all aspects of the root canal system. Additionally, an apically tapered preparation promotes obturation hydraulics while simultaneously controlling and limiting the movement of warm gutta-percha terminally. Improvement in obturation potential is largely attributable to better knowledge and training, as well as the technological advancements in shaping canals, 3-D cleaning, and filling root canal systems (Figure 1).
This article will clinically describe a carrier-based obturation method to fill root canal systems utilizing GuttaCore (Dentsply Sirona). The intention of this article is to inspire clinicians to use a heat-softened, hydraulically effective, and easy-to-learn obturation method. GuttaCore holds the promise to generate “thrill-of-the-fill” experiences and ignite passion in endodontics. If your current obturation method is to insert a cold gutta-percha master cone into a sea of cement, then you are the perfect candidate to switch and, in the same manner, insert a single thermosoftened GuttaCore obturator to the working length, and in 7 to 8 seconds. With the willingness to practice and the desire to improve, you can learn how to predictably fill root canal systems.
Rationale for Filling Root Canal Systems
Dr. Herbert Schilder brilliantly described the biological rationale and mechanical objectives for predictably successful endodontics in 2 internationally acclaimed articles.1,2 These landmark articles describe the essential concepts for anatomical-based shaping, 3-D cleaning, and filling root canal systems (Figure 2). Although the Schilder obturation method has long been the “gold standard” for filling root canal systems, other technologically driven hybrid methods have evolved. Each has been described in different ways and has something to offer, yet all of these methods require a considerable armamentarium, are perceived to be time consuming and technique sensitive, and depend upon a number of ever-changing clinical steps and materials.3
 |
 |
| Figure 1. A working film demonstrates filled root canal systems. The inset image depicts gutta-percha exiting laterally off the body of the shaped canal. | Figure 2. These radiographic images demonstrate minimally invasive shapes and filled root canal systems. (Courtesy of Dr. Herbert Schilder.) |
 |
| Figure 3. These images demonstrate a lesion of endodontic origin and apical corkage utilizing GuttaCore (Dentsply Sirona). The post space was made a few minutes following obturation. (Courtesy of Dr. Shawn Valez, Aiken, SC.) |
Carrier-Based Obturation
In 1978, Dr. William Ben Johnson introduced Thermafil, or a carrier-based obturation method for filling root canal systems.4 Like the Schilder technique, the objective of carrier-based obturation is to carry a wave of warm gutta-percha and sealer along the length of a preparation, starting coronally and ending in apical corkage (Figure 3).5 Today, any given commercially available carrier-based obturator (CBO) has a central carrier, fabricated from either a metal, a polymer, or an all-gutta-percha formulation. Further, the outer skin of any given CBO is comprised of differing formulations of readily flowable gutta-percha. The following will describe the carrier-based obturation method for filling root canal systems, featuring GuttaCore.
Armamentarium
The armamentarium for GuttaCore obturation comprises a pre-selected size verifier and CBO and a heating oven (Figure 4). Additionally, sealer is essential, is a critical lubricant, and should be compatible with any warm gutta-percha technique. Although gutta-percha is the primary bulk material, it is a dimensionally stable and biologically inert sealer that provides an impenetrable seal between the root canal system and the attachment apparatus.
 |
 |
| Figure 4. This image shows a simple armamentarium for filling root canal systems. Note a size verifier, a GuttaCore obturator, and the heating oven. |
Figure 5a. An image showing Pulp Canal Sealer Extended Working Time (PCS EWT) (Kerr) and an evidence-based list of this sealer’s unmatched clinical advantages. |
 |
 |
| Figure 5b. This root canal system was filled utilizing the warm gutta-percha with vertical condensation technique, in conjunction with Kerr PCS EWT. | Figure 6. In this example, when a WaveOne Gold (Dentsply Sirona Endodontics) size 25/07 file is carried to length, the terminus of the canal is gauged with a 25/045 size verifier. The size verifier that is loose at length confirms the correct GuttaCore obturator. |
 |
 |
| Figure 7a. A mechanical file can be converted to a manual file using a clip-on handle. Heat-treatment technology enables easily pre-curving any given file. | Figure 7b. In abrupt apical curvatures, a manual or mechanical motion may be used to subtly adjust the apical extent of any preparation. |
 |
 |
| Figure 8. Any given GuttaCore obturator has circumferential depth control rings on its shaft, which offer a built-in ruler. | Figure 9. The GuttaCore oven has 2 heating chambers. A GuttaCore obturator is hung straight, lowered, and correctly heated by pushing down the elevator button. |
Sealer
More than 70 years ago, Dr. Louis Grossman identified the properties of an ideal root canal sealer.6 Recently, there has been considerable attention focused on bioceramic sealers due to their physical and biological properties. Bioceramic sealers provide prolonged alkalinity over time, which serves to promote bioactivity and antimicrobial behavior. However, this alkalinity is synchronized with solubility, which predisposes to leakage.7 Further problematic, this class of sealers fails to meet Grossman’s criteria, as these materials cannot be dissolved in a solvent, nor be completely removed mechanically, when performing nonsurgical retreatment.8 Yet, like MTA, bioceramic fillers are widely used as root repair materials.
Alternatively, Pulp Canal Sealer Extended Working Time (Kerr) fulfills all of the Grossman requirements for an ideal sealer, has more than 60 years of evidence-based research and clinical success, and can be easily removed when performing retreatment or adhesion dentistry (Figure 5a). Importantly, this sealer is dimensionally stable, biologically inert, and has been shown to have a significantly lower solubility value (P<0.05) compared to bioceramic-based sealers.7 Upon long-term examination, it is reassuring to see a sealer puff associated with a well-filled root canal system vs a sealer puff that has vanished because of solubility (Figure 5b).9,10 The following is a description of the GuttaCore armamentarium.
Size Verifier
Once a canal has been optimally shaped, a size verifier is selected to gauge the terminal diameter of a canal. Typically, the size verifier matches the D0 diameter of the largest shaping file carried to the full working length. Each NiTi size verifier is fluted, has a fixed taper of 0.045 mm/mm, and uses an ISO-colored handle that corresponds to its D0 diameter. When the final shaping file has a taper of 0.04 mm/mm, the GuttaCore obturator selected should have a D0 diameter one size smaller than the largest file taken to the full working length. However, when the final shaping file has a taper of 0.06 mm/mm or greater, the D0 diameters of both the GuttaCore obturator and the largest working file carried to length are typically equal (Figure 6).
The size verifier that can be passively carried to the terminus, and is loose at length, generally confirms the correct GuttaCore obturator to select. Yet, in some instances, the size verifier may be slightly short of length, especially in longer and more curved canals, or canals prepared with small-sized 0.04 tapered files. However, when a shaping file has a taper greater than a size verifier (0.045 mm/mm), the author prefers, when necessary, to manually or mechanically adjust the apical extent of the preparation with the largest heat-treated file that cut its shape to length. Appreciate that NiTi shaping files that are heat-treated are typically far more flexible than a non-heat-treated NiTi size verifier of the same D0 diameter (Figure 7).
 |
 |
| Figure 10a. This radiographic image reveals an endodontically involved posterior bridge abutment. Note the orientation of the prosthesis to the underlying roots. | Figure 10b. This image shows an EndoActivator (Dentsply Sirona) tip distributing an ultrathin layer of sealer along the preparation walls. |
 |
 |
| Figure 10c. This image illustrates removing the silicone stop and handle from a carrier-based obturator (CBO) to facilitate vision when inserting this CBO into any given orifice. | Figure 10d. Note the handle and shaft of this GuttaCore obturator have been broken off at the MB orifice to visually facilitate placing the ML obturator. |
 |
 |
| Figure 10e. This radiographic image demonstrates provisionalization, smooth flowing shapes, and multiple filled apical portals of exit. Note the furcal canal. |
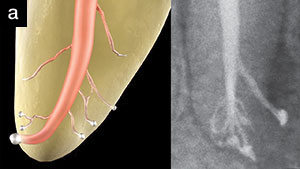
Figure 11a. The graphic animation and mandibular bicuspid both demonstrate filled root canal systems. Note the apical anatomical complexities. |
 |
 |
| Figure 11b. A histologically cleared maxillary bicuspid demonstrates that carrier-based obturation fills root canal systems. SEM demonstrates gutta-percha tags in dentinal tubules. (Courtesy of Giuseppe Cantatore, Rome, Italy.) | Figure 12. This image demonstrates carrier-based obturation of 2 mandibular molars. Note the DB system is filled against the more apically extending DL system. (Courtesy of Dr. Stephen Niemczyk, Drexel Hill, Pa.) |
GuttaCore Obturator
Each GuttaCore obturator utilizes a central cross-linked gutta-percha core. In turn, each core is circumferentially wrapped with a readily flowable, alpha gutta-percha formulation. Like a plugger, the central compacting, all-gutta-percha core is designed to provide sufficient stiffness to capture the maximum cushion of rubber and hydraulically generate an accelerating wave of condensation to the working length. Each obturator has calibration rings that correspond to working depths of 18, 19, 20, 22, and 24 mm on the shaft and 27 and 29 mm on the handle. To improve vision when inserting an obturator into a prepared canal, snip off the rubber stop and simply use the GuttaCore ruler (Figure 8).
Heating Oven
All GuttaCore obturators are thermosoftened on the size 1 heat setting, utilizing either of the 2 heating chambers. The CBO selected is hung straight from the obturator holder by its handle. The heating chamber button is pressed completely down, ensuring that the heating cycle has commenced (Figure 9). In less than 20 seconds, a beep will alert the team that the obturator has been properly heated. Again, press down on the heating chamber button to elevate and access a noticeably heat-softened obturator. Conveniently, the obturator can be left in the oven until it switches off after 90 seconds. This feature provides working time to introduce sealer or place a paper point into an orifice to intentionally block a canal that will be secondarily obturated.
Clinical Technique
Carrier-based obturation is the only filling technique that can simultaneously deliver and compact warm gutta-percha to the terminus of canals that have coronal or mid-root curvatures (Figure 10a). Once a canal has been dried, root canal sealer may be placed using the EndoActivator (EA) (Dentsply Sirona). This is accomplished by pre-fitting an EA tip that is loose 2 mm short of length. The radicular portion of this smooth, flexible, and noncutting polymer tip is lightly “buttered” with sealer, carried into the canal, and activated for about 5 seconds. Gently pumping the EA handpiece serves to uniformly distribute an ultrathin layer of sealer lubricant along the internal walls of the preparation (Figure 10b).
When the GuttaCore oven has completed its heating cycle, the CBO is carefully removed from the oven holder. The shaft of this obturator is then grasped with locking cotton pliers just above the calibration ring that designates the working length. To maximize visibility and control, the handle of the GuttaCore obturator is easily removed by bending it back and forth (Figure 10c). This step allows the obturator, like a paper point, to be carried through the access, inserted directly into the orifice, and slid to length without touching the axial walls. In smoothly prepared canals, the heat-softened obturator is methodically carried to length in about 7 to 8 measured seconds (Figure 10d).
The light inward pressure required to carry a thermosoftened GuttaCore obturator to length serves to both effectively compact warm gutta-percha and offset shrinkage during the cooling cycle.11-13 The central core of a GuttaCore obturator has the desired strength and stiffness to generate an accelerating wave of condensation, starting coronally and ending with apical corkage (Figure 10e). Importantly, the central core, like a piston, provides hydraulics, which compacts warm gutta-percha wall-to-wall, into dentinal tubules, and importantly serves to minimize the sealer interface to 6 to 8 µm.14 Sealer is a critical lubricant that reduces surface tension and enables warm gutta-percha to flow and be compacted laterally and vertically (Figure 11).
There are a couple helpful hints to consider when learning GuttaCore obturation. First, remember to use less sealer than you might otherwise think. Second, when filling 2 canals that apically merge, or that are in close proximity on the pulpal floor, start by placing an ultrathin layer of sealer into both of the dried canals. To maintain vision, place an oversized paper point into the body of the canal not being initially obturated, then trim this paper point coronally. The first GuttaCore obturator is inserted into the open canal and slid to length, and its shaft is removed at the level of the orifice. After removing the paper point, the second GuttaCore obturator is carried apically until it meets resistance, ensuring a 3-D fill (Figure 12).
Following obturation, the pulp chamber should be chemically and/or mechanically cleaned in preparation for restorative dentistry. When a post is deemed necessary, the coronal portion of a GuttaCore obturator can be easily removed because the material is all gutta-percha (Figure 3).15 Appreciate that there are a few clinical situations where a CBO method may be contraindicated, such as certain resorptive defects, open apices, or unshaped canals prepared to dimensions less than a size 20/04 file. Further, cheap files that are subject to excessive heat treatment oftentimes unwind; stretch; and predispose to foraminal rips, tears, and apical transportations. In these instances, MTA or a similarly formulated bioceramic filler may be used to seal root defects.
CLOSING COMMENTS
Effective, controlled, and predictable 3-D obturation is directly related to shaping canals and cleaning root canal systems. With so much interest on minimally invasive endodontics, the increasing trend is minimally invasive instrumentation. Yet, many so-called instrumented canals are neither shaped nor cleaned, and therefore cannot be predictably filled. Anatomically appropriate shaping serves to improve the reservoir of irrigant and, hence, its capacity to penetrate, circulate, and digest tissue from all aspects of the anatomy. 3-D disinfection creates the “opening” for filling a root canal system. With the above in mind, the reader will find GuttaCore obturation simple, fast, and fun and will routinely experience the ethereal thrill-of-the-fill.
References
- Schilder H. Filling root canals in three dimensions. Dent Clin North Am. November 1967:723-744.
- Schilder H. Cleaning and shaping the root canal. Dent Clin North Am. 1974;18:269-296.
- Buchanan LS. Continuous wave warm gutta-percha obturation: using bio-ceramic sealers. Dent Today. 2018;37:86-90.
- Johnson WB. A new gutta-percha technique. J Endod. 1978;4:184-188.
- Cantatore G, Johnson WB. The thermafil system. In: Castellucci A, ed. Endodontics Volume II. Florence, Italy: Il Tridente; 2004.
- Grossman LI. Root Canal Therapy. Philadelphia, PA: Lea & Febiger; 1940:189.
- Poggio C, Dagna A, Ceci M, et al. Solubility and pH of bioceramic root canal sealers: a comparative study. J Clin Exp Dent. 2017;9:e1189-e1194.
- Al-Haddad A, Che Ab Aziz ZA. Bioceramic-based root canal sealers: a review. Int J Biomater. 2016;2016:9753210.
- Casanova F. Understanding Some Clinically Significant Physical Properties of Kerr Sealer Through Investigation [thesis]. Boston, MA: Boston University; 1975.
- Ruddle CJ. Three-dimensional obturation: the rationale and application of warm gutta percha with vertical condensation. In: Cohen S, Burns RC, eds. Pathways of the Pulp. 6th ed. St. Louis, MO: Mosby Yearbook Co; 1994.
- Marlin J, Schilder H. Physical properties of gutta-percha when subjected to heat and vertical condensation. Oral Surg Oral Med Oral Pathol. 1973;36:872-879.
- Tilakchand M, Jain A, Naik B. Expansion of gutta-percha in contact with various concentrations of zinc oxide-eugenol sealer: a three-dimensional volumetric study using spiral computed tomography. J Conserv Dent. 2016;19:317-322.
- Michaud RA, Burgess J, Barfield RD, et al. Volumetric expansion of gutta-percha in contact with eugenol. J Endod. 2008;34:1528-1532.
- Ruddle CJ. An In Vitro Scanning Electron Microscope Study of the Warm Gutta Percha With Vertical Condensation Technique [thesis]. Boston, MA: Harvard School of Dental Medicine; 1976.
- Ruddle CJ. Ruddle on Retreatment [DVD]. Santa Barbara, CA: Advanced Endodontics; 2004.
Dr. Ruddle is founder and director of Advanced Endodontics, an international educational source, in Santa Barbara, Calif. He is an assistant professor of graduate endodontics at Loma Linda University and the University of California, Los Angeles; an associate clinical professor at the University of California, San Francisco; and an adjunct assistant professor of Endodontics at the University of the Pacific School of Dentistry. As an inventor, Dr. Ruddle has designed and developed several instruments and devices that are widely used internationally. He is well known for providing endodontic education through his lectures, clinical articles, training manuals, videos, and DVDs. Additionally, he maintains a private practice in Santa Barbara, Calif. He can be reached at (800) 753-3636 or at the website endoruddle.com.
Disclosure: Dr. Ruddle has a financial interest in products on which he collaborates, which includes The EndoActivator System.
Related Articles
The Shaping Movement: Fifth-Generation Technology
Focus On: Endodontic Emergencies
Broken Instrument Removal: The Endodontic Challenge








