Overcoming the Limitations of Conventional Impressions With Intraoral Scanning and Grammetry
Written by: Drs. John Heimke and Gregori M. Kurtzman
INTRODUCTION
Full-arch implant rehabilitation requires a level of precision that exceeds the demands of single-tooth or short-span treatment. The accuracy of the impression phase directly influences prosthesis fit, restorative success, and long-term patient outcomes. Conventional impression techniques, while reliable, are being increasingly replaced by digital alternatives, such as intraoral scanning (IOS) and grammetry. These technologies streamline workflows, improve accuracy, and enhance communication with the laboratory, ultimately benefiting both the clinician and the patient.
Elastomeric (physical) impression materials, including polyvinyl siloxane and polyether, are susceptible to polymerization shrinkage, distortion during tray removal, and dimensional changes during storage or disinfection.1 Regarding full-arch treatment, small inaccuracies accumulate, leading to clinically significant prosthetic misfit. Tray stability is also problematic in edentulous arches, with even splinted impression copings vulnerable to micromovement.2,3 Verification jigs (stents) are often required to confirm cast accuracy, adding chair time and additional appointments.4 Those verification jigs aid in eliminating implant impression abutment movement that may result in relation to the implants with each other on the arch being captured.5 From the patient’s perspective, conventional impressions are bulky, uncomfortable, and often associated with gagging, diminishing the treatment experience.
Benefits of Intraoral Scanning and Grammetry
IOS eliminates the need for impression materials and trays, capturing digital data directly and allowing real-time assessment of scan quality. Errors can be corrected immediately without repeating the entire process, improving workflow efficiency and patient comfort. Digital files are stable, easily archived, and seamlessly integrated into CAD/CAM workflows.6
Photogrammetry further enhances precision in full-arch cases by capturing the exact 3D spatial relationship of implants. Using coded scan bodies and extraoral imaging, implant positions can be recorded with micro accuracy, which is independent of soft-tissue distortion or arch length.7 Unlike traditional verification methods, photogrammetry transfers implant coordinates directly into the digital workflow, reducing errors and expediting prosthetic fabrication.
When combined, IOS provides soft-tissue and occlusal detail, while photogrammetry ensures accurate implant positioning. This synergy reduces the number of analog steps, shortens treatment timelines, and increases predictability. Patients benefit from fewer visits, faster delivery, and a more comfortable experience.8 A digital workflow significantly improves communication between the clinician and the laboratory. With IOS, detailed impressions can be transmitted instantly, eliminating risks of distortion associated with shipping physical impressions or pouring models. Lab technicians can review scans in real time and request modifications before beginning fabrication. Photogrammetry complements IOS by providing accurate implant coordinates, enabling frameworks and prostheses to be virtually designed with confidence. A fully digital pathway allows frameworks and provisionals to be designed, milled, or 3D printed with greater consistency, enhancing passive fit and long-term stability. Additionally, cloud-based platforms further enhance collaboration, enabling seamless sharing of case data, designs, and aesthetic simulations. This fosters interdisciplinary planning and ensures restorative outcomes align with patient expectations.
Clinical Benefits of an Intraoral Scanner
The Medit i900 (Medit) is the newest model in the company’s i-series and reflects continued refinement in speed, accuracy, and usability. It incorporates hardware and software upgrades that improve clinical efficiency and case predictability in restorative and implant dentistry. Ergonomically, the i900 is lightweight and balanced, paired with a thinner, more flexible cable that improves handling and reduces fatigue during extended use. A larger field of view and redesigned scan tips enhance access in posterior areas, simplifying margin capture and minimizing stitching errors that can compromise accuracy in full-arch scans.
A significant advantage of the i900 lies in its open architecture. The system is fully compatible with several CAD platforms, including exocad (exocad), one of the most widely adopted CAD platforms in dentistry. This integration allows seamless transfer of scan data directly into restorative and implant planning workflows. For the clinician, it eliminates conversion steps and reduces the potential for file errors. For the laboratory, exocad compatibility simplifies design and fabrication, shortening turnaround times and improving communication between the treating dentist and the technician. The net result is a more efficient digital workflow that benefits both provider and patient.
Application of Grammetry for Full-Arch Implant Rehabilitation
Grammetry has emerged as a valuable tool in digital implant dentistry, particularly for full-arch rehabilitation where passive fit is critical to long-term success. Traditionally, photogrammetry required dedicated systems with specialized hardware, adding cost and complexity to the workflow. The Medit i900, with its high-resolution optics and advanced image-stitching algorithms, expands the utility of an intraoral scanner by enabling photogrammetry-based workflows without the need for separate equipment.
The scanner’s wide field of view and enhanced tracking accuracy allow capture of multiple implant positions with precision comparable to dedicated photogrammetry systems. This is particularly relevant when scanning multi-unit implant restorations, where even minor deviations can result in misfit and biologic or mechanical complications. By combining intraoral scans of the implants and soft tissues with extraoral scans of the prosthetic components, the i900 supports a fully digital pathway from data capture to prosthesis design.
While the i900 demonstrates accuracy suitable for photogrammetry in clinical practice, limitations remain in certain situations. Subgingival implant positions, bleeding, or soft-tissue interference may affect scan quality, highlighting the importance of proper tissue management and scanning protocols. Despite these considerations, the ability to perform photogrammetry with a multifunctional intraoral scanner such as the i900 represents a significant advancement, broadening access to precision digital workflows in implant dentistry.
Clinical Applications in Digital Dentistry
Facially driven treatment planning has become an integral component of restorative and implant dentistry, enabling clinicians to harmonize prosthetic design with the patient’s natural aesthetics. The RayFace system (Ray America) represents an advancement in extraoral 3D facial scanning, providing rapid, high-resolution capture of facial structures that can be directly integrated into digital workflows. Unlike conventional 2D photography, which limits visualization to static planes, RayFace produces a dynamic 3D dataset, permitting evaluation of symmetry, lip mobility, smile line, and soft-tissue contours.
The scanner’s design emphasizes both accuracy and efficiency. Full-face acquisition requires only a few seconds, reducing patient movement artifacts and improving the reliability of the digital file. Integration with CAD software such as exocad allows alignment of intraoral scans and facial data. Enabling prosthetically driven implant positioning and restorative design that reflect both function and aesthetics. This is particularly advantageous in full-arch rehabilitation, where tooth or implant position and occlusal plane must be considered within the context of facial balance.
For the clinician, the ability to merge intraoral and facial scans reduces the guesswork inherent in analog smile design and enhances communication with the dental laboratory. Patients benefit from improved visualization of proposed outcomes, facilitating case acceptance by allowing them to preview potential aesthetic results before treatment begins.
Full-Arch Scanning and the Lab
Full-arch implant rehabilitation requires a level of scanning precision that exceeds the demands of single-tooth or short-span restorations. Two recent innovations, SmartX-ScanLadder (Medit) and ArchBridge (ROE Dental Laboratory), address those challenges from complementary but distinct directions.
The SmartX-ScanLadder, is a software-driven guided scanning protocol integrated into the Medit platform. It provides a visual “laddered” pathway across the arch during intraoral scanning, directing the clinician to follow a structured sequence of image acquisition. By standardizing the order and orientation of scans, SmartX-ScanLadder reduces stitching drift, minimizes incomplete data sets, and shortens rescanning time. Its role is to guide the sequence of scan acquisition, ensuring efficiency and consistency in the digital workflow.
In contrast, the ArchBridge, is a hardware-assisted accessory designed to improve cross-arch accuracy. The device connects implant scan bodies with a rigid cross-arch framework, stabilizing the spatial relationship between implants during scanning. This physical connection enhances the fidelity of long-span data capture, reducing distortion across the arch, and delivering a more accurate digital file to the laboratory. Its role is to improve the accuracy of cross-arch relationships, which directly translates into a better-fitting prosthesis and fewer intraoral adjustments at delivery.
When combined, the 2 systems work synergistically: SmartX-ScanLadder (software-driven) ensures the scan is captured in the proper sequence, while ArchBridge (hardware-assisted) stabilizes and validates the cross-arch implant relationships. For clinicians, this integration reduces chair time and enhances confidence in the digital impression. For patients, it shortens appointments and improves comfort. And for laboratories, it results in cleaner, more reliable datasets that streamline CAD/CAM design and fabrication.
Case Presentation
A 70-year-old male patient presented for consultation regarding a loose maxillary tooth (No. 8) and a recently lost tooth (No. 7) (Figure 1). Examination noted fair oral hygiene with light generalized bleeding and teeth Nos. 1 to 4, 7, 12, 14 to 16, 18 to 20, 29, and 30 missing. The maxillary teeth had existing veneers present and a 3-unit bridge on Nos. 11 to 13. A CBCT was taken to evaluate the anatomy and bone. A panoramic view noted a large periapical lesion on tooth No. 5, with bone loss on the remaining maxillary teeth (Figure 2). Bone loss was also noted on the 2 remaining mandibular molars (Nos. 17 and 31). Evaluation of the CBCT in 3D views revealed dehiscence of the remaining maxillary dentition, making those teeth poor candidates to be retained (Figure 3). Treatment options were discussed with the patient, who indicated he wished to address the maxillary arch at this time and the mandibular arch at a later time. Treatment for the maxillary arch would consist of extracting the remaining maxillary teeth and placing implants for an All-on-4 approach. The posterior implants would be angled bilaterally to skirt the mesial maxillary sinus wall and avoid the need for sinus augmentation. The implant platforms would be placed at Nos. 3, 6, 10, and 13. A provisional hybrid would be placed approximately 72 hours later. The patient agreed to the presented treatment plan, and treatment would be coordinated with an oral surgeon.



To initiate planning, a dynamic video was taken of the patient, and a 3D face scan was performed using RayFace (Figure 4), as well as intraoral scanning with the Medit i900 IOS unit (Figure 5). The data was transmitted to ROE Dental Laboratory, including the CBCT for fabrication of a virtual full arch that would allow a surgical guide to be fabricated to guide implant placement based on the anatomy. The patient was scheduled for implant surgery with the oral surgeon.


ROE Dental Laboratory, with input from the lead author, virtually set up the maxillary arch, maintaining the incisal length of the current dentition. A clear maxillary denture was designed with an occlusal/palatal channel to position the implants to exit the ridge in that area. That guide was then printed on the UltraCraft A series 3D printer (HeyGear) in high-strength clear resin (Keystone Industries) (Figure 6). The surgical guide was sent to the practice for the surgical appointment.

The patient presented for a surgical appointment at the oral surgeon’s office, accompanied by the lead author, who documented the case and captured digital records for the fabrication of an immediate provisional hybrid prosthesis, which was to be delivered the following day. The consent form was reviewed by the patient and signed. Local anesthetic was administered across the maxilla.
Two fiduciary markers were placed at the midpalate prior to intraoral scanning to provide a stable reference point with the Medit IOS to align grammetry scans (Figure 7). The maxillary dentition was extracted. A mid-ridge incision was made from the right tuberosity to the left tuberosity, and a full-thickness flap was elevated to expose the ridge. The extraction sockets were curetted to remove any residual tissue. The clear surgical guide was tried in to verify seating on the arch and the patient was guided into occlusion to confirm it was positioned aesthetically (Figure 8, left). Osteotomies were created at the planned positions with the emergence of the implant platforms at the mid-ridge (Figure 8, right). The guide was utilized to position MUAs (multi-unit abutments) on each implant, with 30° on the posterior implants and 17° on the anterior implants, to ensure they exited within the channel on the guide (Figure 9). ArchBridge ScanBodies were placed on the MUAs, ready for a second grammetry scan (Figure 10). A new scan was completed with the Medit i900 IOS. Wide-body, mushroom-shaped healing caps were placed on the implants, followed by suturing the flaps in preparation for the third and final grammetry scan, which was completed (Figure 11).





The data was transmitted to ROE Dental Laboratory to utilize their same-day grammetry design services and fabricate a provisional hybrid prosthesis. The lab, using the virtual setup that was used to fabricate the abutment guide, designed the provisional hybrid in exocad. The provisional prosthesis was 3D printed (Carbon M3 Max printer) with high-strength Lucitone Digital print resin (Denstply Sirona). Following finishing, Optiglaze (GC America) was applied to characterize the pink gingival aspect.
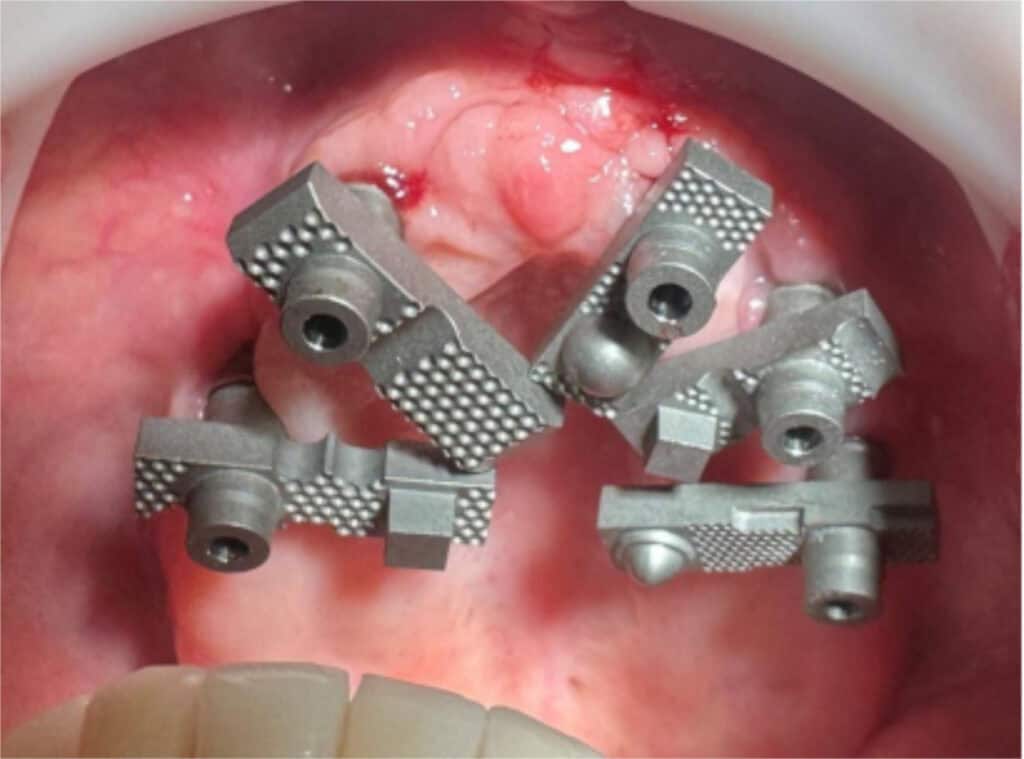
The patient returned after 72 hours, and the mushroom healing caps were removed. A provisional hybrid was then tried in to verify that it was properly seated on all implants. A panoramic radiograph was taken to verify prosthesis seating (Figure 12). The patient was scheduled for recall to check healing and placed on a regular schedule while the implants were osseointegrating. At 3 months post-implant placement and provisionalization the hybrid was removed intraorally, and it was noted that the implant at site No. 10 was mobile, indicating it had failed to osseointegrate. Local anesthetic was administered, and the failing implant was removed. Additional implants were placed at site Nos. 9 and 11. Healing abutments were then placed, and the provisional hybrid was reinserted to allow healing of the new implants. The patient returned 12 weeks later to initiate the final restorative phase of treatment. The provisional hybrid was removed, and the healing abutments on the 2 new implants were replaced with 17° MUAs (Figure 13). A panoramic radiograph was taken of the MUAs in all the implants on the maxillary arch (Figure 14). Temporary cylinders were placed on the MUAs, and measurements were taken with a caliper (Figure 15). Based on the measurements between the implants, a Fast Protect Easy Bar (XPdent Corp) was placed connecting the implants. The Easy Bar components were connected with Stellar resin (Taub Products) to create an index, which was removed intraorally to create a passive fit implant verification jig for the lab to fabricate a printed provisional hybrid and the final zirconia hybrid restoration (Figure 16). Mushroom-shaped healing abutments were placed on all the abutments, and an IOS was taken with the Medit i900 scanner (Figure 17). Those abutments were then removed, and ScanLadder scan bodies were placed on the implants in preparation for grammetry (Figure 18). The scan bodies were removed intraorally, and the original provisional that had been removed at that appointment was reinserted intraorally, and the patient was dismissed.






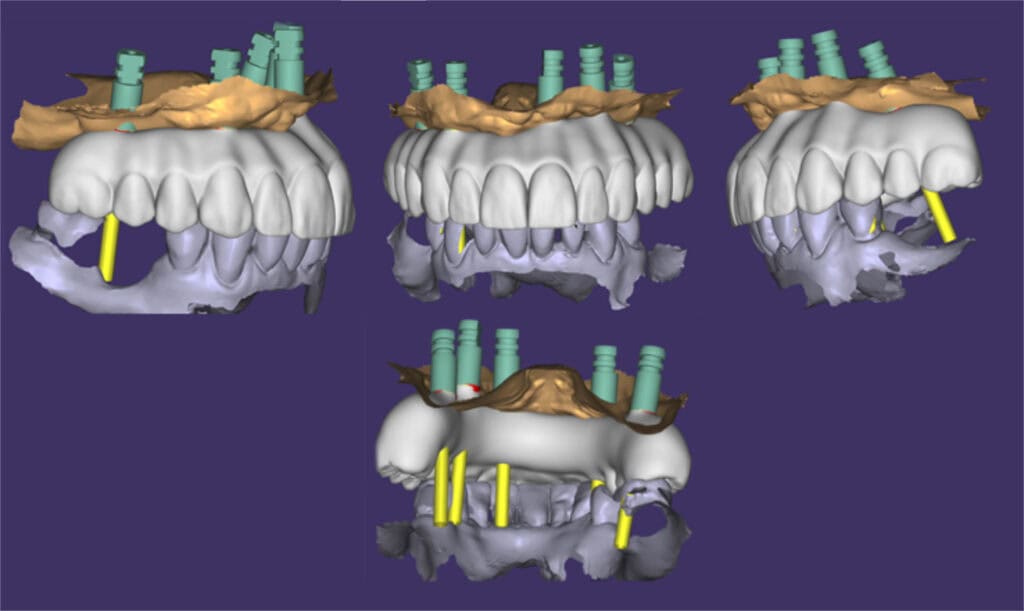
The IOS and grammetry data were transmitted to the lab, which was then imported into exocad to fabricate a new provisional hybrid prosthesis (Figure 19). The lab tech added the new scans into the virtual design from which the original prosthesis was fabricated. The new provisional prosthesis was designed to accommodate the 5 implants present on the maxilla (Figure 20). The prosthesis was then printed on the Carbon printer unit using high-strength resin. As with the original provisional, hybrid gingival coloration was added to complete the prosthesis (Figure 21). The patient returned, and the old provisional hybrid was removed, and the new hybrid was inserted. The occlusion was checked, and the patient indicated he was happy with the aesthetics (Figure 22).



The patient confirmed that he was satisfied with the aesthetics and did not want any changes. The patient confirmed the shade with custom zirconia shade tabs and signed off to proceed to the final stage. This was communicated to the lab to fabricate the final zirconia hybrid, which replicates the form, aesthetics, and occlusion of the recent provisional.
The final zirconia hybrid was fabricated with Bespoke (ROE Dental Laboratory), a line of premium full-arch restorations. These hybrid restorations combine over 40 points of customization, innovative materials, and skilled artisanship to create a totally unique prosthesis tailored to each individual patient. The final Bespoke zirconia hybrid was milled in the CORiTEC 350i series (imes-icore GmbH) using an ArgenZ Multilayered puck (Argen) and beautified using MiYO liquid ceramic (Jensen Dental) (Figure 23).

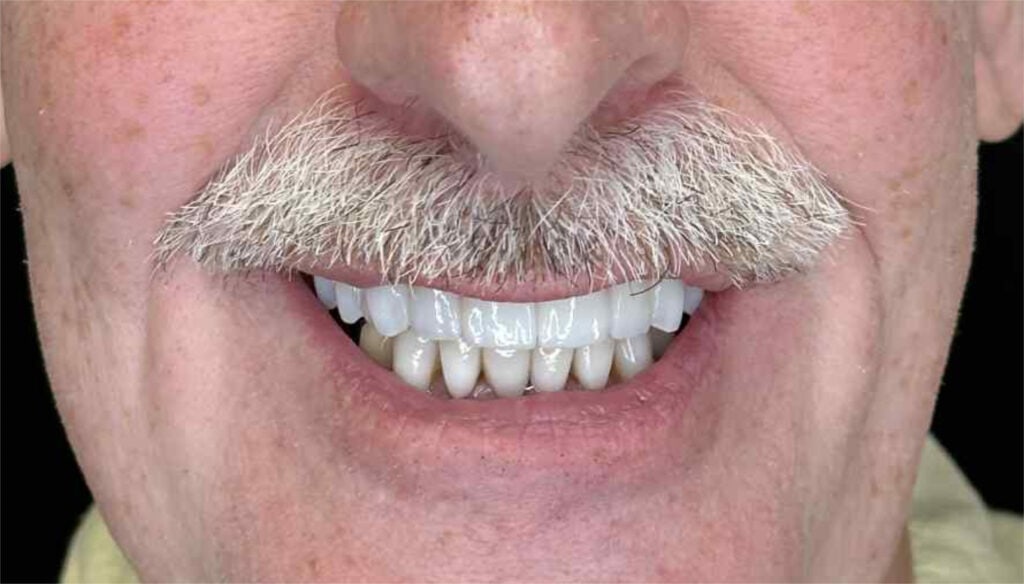
The patient presented, and the provisional hybrid was removed. The final Bespoke zirconia hybrid was inserted intraorally and Dess Torx screw for Straumann MUA screws were tightened to 35 Ncm per the recommended torque. A panoramic radiograph was taken to verify complete seating of the prosthesis to the implants MUAs (Figure 24). Occlusion was verified, and no adjustments were required. The screw access holes were filled with Teflon tape and sealed with LuxaFlow composite (DMG America). The patient was given a mirror to check the aesthetics, which matched the prior provisional hybrid, and he expressed he was happy with the results (Figure 25). The result was a natural smile (Figure 26).


CONCLUSION
The shift from conventional impressions to digital workflows in full-arch implant rehabilitation reflects broader trends in dentistry toward efficiency, accuracy, and patient-centered care. The evidence consistently demonstrates that IOS provides accuracy comparable to or superior to elastomeric impressions in short spans, and when combined with grammetry, can achieve the precision necessary for full-arch prostheses. The clinical implications are significant. Reduced reliance on verification jigs and fewer prosthetic complications translate into shorter treatment timelines and improved patient satisfaction. Furthermore, digital records are easily stored and retrieved, simplifying maintenance, repair, and future treatment planning.
The advantages in accuracy, efficiency, and collaboration position IOS and grammetry as transformative tools in implant dentistry. As the technology becomes more accessible and user-friendly, broader adoption is likely, with direct benefits for both patients and clinicians alike. Conventional impressions, while once the standard, are limited by material instability, technique sensitivity, and patient discomfort—limitations that are magnified in full-arch implant cases. Intraoral scanning and grammetry overcome these challenges, improving accuracy, patient experience, and efficiency. By enhancing laboratory communication and enabling fully digital fabrication, these technologies are redefining the standard of care in full-arch implant rehabilitation.
REFERENCES
- Djurovic Koprivica D, Puskar T, Budak I, et al. Influence of implant impression methods, polymer materials, and implant angulation on the accuracy of dental models. Polymers (Basel). 2022;14(14):2821. doi:10.3390/polym14142821
- Assunção WG, Cardoso A, Gomes EA, et al. Accuracy of impression techniques for implants. Part 1—Influence of transfer copings surface abrasion. J Prosthodont. 2008;17(8):641–7. doi:10.1111/j.1532-849X.2008.00308.x
- Alikhasi M, Siadat H, Beyabanaki E, et al. Accuracy of implant position transfer and surface detail reproduction with different impression materials and techniques. J Dent (Tehran). 2015;12(10):774–83.
- Papaspyridakos P, Lal K, White GS, et al. Effect of splinted and nonsplinted impression techniques on the accuracy of fit of fixed implant prostheses in edentulous patients: a comparative study. Int J Oral Maxillofac Implants. 2011;26(6):1267–72.
- Schneider A, Kurtzman GM, Silverstein LH. Improving implant framework passive fit and accuracy through the use of verification stents and casts. J Dent Technol. 2001;18(4):23–5.
- Mangano FG, Veronesi G, Hauschild U, et al. Trueness and precision of four intraoral scanners in oral implantology: a comparative in vitro study. PLoS One. 2016;11(9):e0163107. doi:10.1371/journal.pone.0163107
- Beri A, Pisulkar SK, Bagde AD, et al. Evaluation of accuracy of photogrammetry with 3D scanning and conventional impression method for craniomaxillofacial defects using a software analysis. Trials. 2022;23(1):1048. doi:10.1186/s13063-022-07005-1
- Alfaraj A, Alqudaihi F, Khurshid Z, et al. Comparative analyses of accuracy between digital and conventional impressions for complete-arch implant-supported fixed dental prostheses—A systematic review and meta-analysis. J Prosthodont. doi:10.1111/jopr.14094
ABOUT THE AUTHORS
Dr. Heimke is a 1989 graduate of Case Western Reserve University School of Dental Medicine (DMD), also earning a graduate degree, Masters in Public Health (MPH) from Emory University. He completed a residency program in general dentistry at Ft. Benning, Ga., while serving in the U.S. Army. He is in private practice in Cleveland, OH. He is a Fellow of the Academy of General Dentistry, Dr Heimke is a member of the Oral Design, founded by Mr Willi Geller, MDT, Zurich, Switzerland, a DentalXp expert/lecturer, visiting faculty at the FMR NYC program, and International lecturer on Digital Smile Design, Cosmetic Dentistry, Digital Dentistry Workflows, Full Arch Implants, Marketing, and Case Acceptance. He can be reached at [email protected].
Dr. Kurtzman is in private general dental practice in Silver Spring, Maryland, USA and a former Assistant Clinical Professor at University of Maryland in the department of Restorative Dentistry and Endodontics and a former AAID Implant Maxi-Course assistant program director at Howard University College of Dentistry. He has lectured internationally on the topics of Restorative dentistry, Endodontics and Implant surgery and prosthetics, removable and fixed prosthetics, Periodontics and has over 920 published articles globally, several ebooks and textbook chapters. Dr. Kurtzman has been honored to be included in the “Top Leaders in Continuing Education” by Dentistry Today annually since 2006 and was featured on their June 2012 cover. He can be reached at [email protected].