
Written by: Drs. George Athansios, Annemarie O. Athansios, Allen Honigman, Howard Drew, Emil Cappetta
In today’s aesthetic society, dental professionals perform extensive therapies to achieve smile harmony. Procedures focus on the shape, position, and color of the teeth, as well as the position and contours of the free gingival margin and papillae. The “gummy” smile has been treated through orthognathic surgery and lip repositioning operations. Historically, minimal therapy has been used to address aesthetically unpleasing pigmentation of the gingiva. Most patients and clinicians are unaware of the depigmentation procedure and its ability to address aesthetic issues, such as irregular coloring and pigmented “spots” on the tissues. This article will discuss the history, histology, and physiology of pigmentation. Treatment modalities will be discussed along with the physics and rationale for the use of digitally pulsed Nd: YAG laser depigmentation therapy. Clinical cases will be presented depicting the benefits of this technique.
INTRODUCTION
The harmony of a smile is determined by multiple factors: shape, position, and color of the teeth, as well as gingival appearance.1 Pigmented gingiva is not pathologic, but it may present an aesthetic concern to many individuals, especially when the patient has a “gummy smile” or excessive gingival display. Most of the patients, as well as a part of the dental community, are often not well educated about the options available to treat these aesthetic concerns and that depigmentation is a viable therapy.2
Pigmentation of the mucosa has been observed and described since the early 1900s. Many reports demonstrate it to be associated with different races, such as Filipinos, French, Arabians, Chinese, East Indians, and African Americans. Even though physiologic pigmentation is most likely dictated by genetics, oral pigmentation can occur in all races.2 Darker gingival pigment can be caused by a variety of physiological processes and physical conditions. Environmental factors, as well as smoking, ethnicity, and race, have been seen as major factors contributing to the color of the gingiva.3,4 Physiologic pigmentation of the oral mucosa is manifested clinically as multifocal or diffuse melanin pigmentation with variable prevalence in different ethnic groups. Melanin is the most common natural pigment contributing to the endogenous pigmentation of the gingiva.5 This brown pigment formed by melanocytes, dendtritic cells of neuroectodermal origin located in basal and suprabasal layers of gingival epithelium. It is currently known that they are capable of dividing and maintaining themselves, hence, self-reproduce.6 The physiology of melanocytes shows a structure that has a round base with a pale staining cytoplasm that populates the epidermis. These cells lack attachment structures such as desmosomes and associated with them keratin intermediate tonofilaments. Instead, melanocytes possess long dendritic processes. These dendritic processes make it possible for melanocytes to contact other cells over distances. Melanocytes are capable of synthesizing an amino acid tyrosine that initiates the events leading to the synthesis and deposition of melanin.5
The elimination of benign pigmented lesions can be treated with various modalities with different results.7 Chemical agents such as 90% phenol and 95% alcohol have been used in the past, but many clinicians stopped using them due to side effects on the soft gingival tissue.8 Free autogenous soft tissue graft surgery is another modality. However, this technique is associated with higher morbidity due to an additional surgical site, and often, color-matching aesthetics is a concern.9 Abrasion methods with diamond burs operating on a high-speed handpiece have also been described in the literature, but the challenge for this modality was to control the depth of de-epithelialization and maneuverability of handpiece.10
In today’s world, selective removal of pigmented gingivae by lasers is becoming increasingly popular as the process proves to be less traumatic and aesthetically attractive. The objective of this study was to evaluate and explore the treatment outcomes of the Nd:YAG laser wavelength 1064 nm for gingival depigmentation. The pulsed Nd:YAG laser (Periolase MVP-7 [Millenium Dental Technologies, Inc) was used because its wavelength of 1064 nm is highly absorbed in pigmented tissue with an additional benefit of not damaging the underlying connective tissue layer.11 The article demonstrated that gingival harmonious color was necessary to achieve total smile aesthetics. The data presented in the article should help educate the public and dental professionals on how essential this procedure is.
MATERIALS AND METHODS
The study was designed as a retrospective nonconsecutive case series. Three patients (1 male and 2 females) with high aesthetic concerns presented to the dental clinic at Rutgers School of Dental Medicine (RSDM) (Figures 1 to 3). As a part of comprehensive care evaluation, when patients stated that they were unhappy with their smile, then they were questioned if gingival color harmony was a part of their aesthetic complaint. If one of their chief complaints was to improve upon the gingival color due to the nonuniform pigmentation and/or a lack of smile harmony, they were offered to have a gingival depigmentation laser procedure. To maintain consistency between cases, only 2 residents under the supervision of specific faculty were selected to perform the procedure. This case series has been reported in line with the PROCESS Guideline.
CASE 1
A 32-year-old male patient reported to the Department of Periodontology, RSDM, with a complaint of gingival pigmentation upon smiling. The patient did not have any significant medical history and was classified as ASA 1. Dental examination revealed a high smile line12 and heavy bilateral gingival pigmentation (Dummett–Gupta oral pigmentation index [DOPI]).13,14 Intraoral pictures were taken, and treatment options were discussed and explained to the patient.
Surgery
The treatment was rendered using digitally pulsed Nd:YAG laser (Periolase MVP-7) by one of the second-year residents under the direct supervision of the faculty. After achieving local anesthesia, the laser was employed in contact mode using 3.6 W, 100 µsec, and 20 Hz. Depigmentation was performed using the laser tip horizontally and parallel to the axis of the teeth in contact with the pigmented part of the gingiva. The patient was given postoperative oral hygiene instructions along with chlorhexidine mouthwash and recalled at 2 and 4 weeks post-op. Final photograph was taken at one of the oral prophylaxis appointments 13 months after treatment (Figure 1).

CASE 2
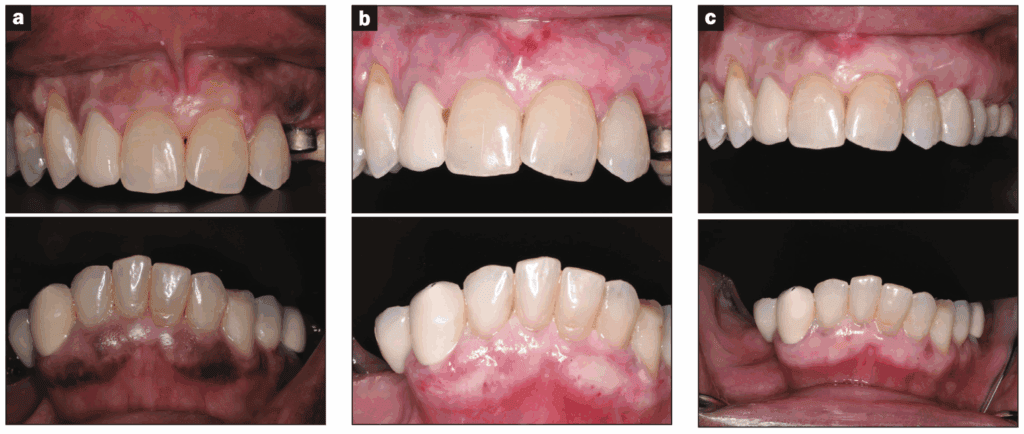
A 63-year-old female patient reported to the Department of Periodontology, RSDM, with a complaint of pigmented gums. The patient was classified as ASA 2 patient due to a history of controlled hypertension. Dental examination revealed moderate bilateral gingival pigment with mixed pink and brown gingiva according to DOPI (Figure 2a) and a high smile line.12 Intraoral pictures were taken, and treatment with Nd:YAG laser wavelength was performed following the surgical steps as described in Case 1. Clinical photographs were taken at 1-week and 8-month postsurgical followup (Figures 2b and 2c).
CASE 3
A 45-year-old female patient reported to the Department of Periodontology, RSDM, with a complaint of not liking her smile. The medical history was insignificant, and dental examination revealed uneven moderate gingival pigment (DOPI)13 (Figure 3a). Intraoral pictures were taken, and surgical steps utilizing the digitally pulsed Nd-YAG laser were performed as described in Case 1. Clinical photographs were taken before and during the surgery (Figures 3a and 3b) and postsurgically at 4-week followup (Figure 3c) and 1-year followup (Figure 3d).

RESULTS
All patients had several followup appointments. All 3 cases were seen 2 weeks after the procedure and reported minimal to no discomfort postsurgically. No spontaneous bleeding or impaired wound healing was observed or reported by the patients. All cases demonstrated a significant reduction in pigmentation levels at all sites. Patients’ aesthetic expectations were met in all cases as measured by patient post-op satisfaction questions.
DISCUSSION
It is imperative to realize that laser affects tissue in 4 different ways: absorption, reflection, transmission, and scatter. Absorption depends on the wavelength, tissue composition, water content, and pigmentation. Melanin is best absorbed at a wavelength close to 1000 nm.2 The Nd-YAG wavelength of 1064 nm is highly absorbed by the pigmented tissue, making it a very effective surgical laser for cutting and coagulating dental soft tissues, with the additional benefit of good hemostasis.
This article aimed to evaluate and explore the efficacy of the digitally pulsed Nd-YAG laser in achieving gingival color harmony and aesthetics in patients who desire to undergo gingival depigmentation treatment. Four patients with aesthetic concerns of gingival pigmentation were treated with ND:Yag laser to remove melanin pigmentation at RSDM.
No side effects were reported, and the texturing of gingivae appeared to return to match the non-pigmented gingivae in the oral cavity. More importantly, patients reported no post-op pain or discomfort, with minimal to no downtime during the healing process.
In considering the current applications for the advancement of the laser-assisted depigmentation techniques, further studies and research will be necessary to enhance treatment prognosis and predictability. While gingival melanin pigmentation can result from local, systemic, environmental, or genetic factors, it is important to consider the etiology in every case. Ensuring treatment success requires identifying and eliminating the potential causative agent of pigmentation before proceeding with surgical treatment. Lasers, particularly Nd:YAG, seem to offer the least recurrence or pigmentation with limited morbidity.
CONCLUSION
In the past, gingival color harmony has rarely been considered by patients and dentists. Depigmentation of gingival melanin by a digitally pulsed Nd:YAG laser is a safe and efficacious procedure. Patient healing was prompt and pain-free, yielding very aesthetic results. As the future of laser treatment continues to evolve, we anticipate fewer relapses and achieve even better results.
Laser depigmentation to achieve gingival color harmony can be a valuable addition in fulfilling the demands of an aesthetically pleasing smile. The article demonstrated that gingival color harmony should be included in achieving ideal smile aesthetics. The data presented in the article should help educate the public and dental professionals on the importance of laser depigmentation procedures for achieving aesthetic results.
Dr. Neal Lehrman passed away prior to publication in January at the age of 56. He was a devoted father. To his friends and colleagues, he was a brilliant person who spoke passionately about laser therapy. Neal was trained in periodontics and implantology at Rutgers School of Dental Medicine and remained an adjunct assistant professor at the institution. He was a pioneer in laser dentistry, always presenting new procedures in regeneration, depigmentation, wound healing, and BRONJ. He was revered by his students and colleagues and was always available to teach and instruct everyone. His brilliance was only overshadowed by his sense of humor and his love of his family.
REFERENCES
1. Deepak P, Sunil S, Mishra R, et al. Treatment of gingival pigmentation: a case series. Indian J Dent Res. 2005;16(4):171–6. doi:10.4103/0970-9290.29901
2. Grover HS, Dadlani H, Bhardwaj A, et al. Evaluation of patient response and recurrence of pigmentation following gingival depigmentation using laser and scalpel technique: A clinical study. J Indian Soc Periodontol. 2014;18(5):586–92. doi:10.4103/0972-124X.142450
3. Dover JS, Smoller BR, Stern RS, et al. Low-fluence carbon dioxide laser irradiation of lentigines. Arch Dermatol. 1988;124(8):1219–24.
4. Hedin CA. Smokers’ melanosis. Occurrence and localization in the attached gingiva. Arch Dermatol. 1977;113(11):1533–8. doi:10.1001/archderm.113.11.1533
5. Yamaguchi Y, Hearing VJ. Melanocytes and their diseases. Cold Spring Harb Perspect Med. 2014;4(5):a017046. doi:10.1101/cshperspect.a017046
6. Hearing VJ. Determination of melanin synthetic pathways. J Invest Dermatol. 2011;131(E1):E8-E11. doi:10.1038/skinbio.2011.4
7. Chatterjee A, Singh N, Malhotra P, et al. Gingival pigmentation and its treatment modalities. J Dent Scie Oral Rehab. 2011;2:11–4.
8. HIRSCHFELD I, HIRSCHFELD L. Oral pigmentation and a method of removing it. Oral Surg Oral Med Oral Pathol. 1951;4(8):1012–6. doi:10.1016/0030-4220(51)90448-3
9. Tamizi M, Taheri M. Treatment of severe physiologic gingival pigmentation with free gingival autograft. Quintessence Int. 1996;27(8):555–8.
10. Murthy MB, Kaur J, Das R. Treatment of gingival hyperpigmentation with rotary abrasive, scalpel, and laser techniques: A case series. J Indian Soc Periodontol. 2012;16(4):614–9. doi:10.4103/0972-124X.106933
11. Gross AJ, Herrmann TR. History of lasers. World J Urol. 2007;25(3):217–20. doi:10.1007/s00345-007-0173-8
12. Tjan AH, Miller GD, The JG. Some esthetic factors in a smile. J Prosthet Dent. 1984 Jan;51(1):24-8. doi: 10.1016/s0022-3913(84)80097-9. PMID: 6583388.
13. Dummett CO, Bolden TE. Postsurgical clinical repigmentation of the cingivae. Oral Surg Oral Med Oral Pathol. 1963;16:353–65. doi:10.1016/0030-4220(63)90299-8
14. Dummet CO, Gupta OP. Estimating the epidemiology of oral pigmentation. J Natl Med Assoc. 1964;56(5):419–20.
ABOUT THE AUTHORS
Dr. Athansios earned his DMD at Rutgers School of Dental Medicine (RSDM), formally UMDNJ, and soon after, practiced as a general dentist for 14 years. After becoming a Fellow of the American Academy of General Dentistry, a Fellow of the American Academy of Implant Dentistry, and a Diplomate of the American Board of Oral Implantology, Dr. Athansios returned to RSDM to complete his periodontal residency. Today, Dr. Athansios is an active member of the American Academy of Periodontology, American Dental Association and New Jersey Dental Association (NJDA). He is a past president of the Essex County Dental Society and currently sits as a Trustee on the Board of NJDA. He is a volunteer firefighter and actively participates on mission trips with colleagues to provide dental treatment to underprivileged communities around the world. Dr. Athansios has participated on missions to Egypt, Ethiopia, and Bolivia. Dr. Athansios has a private practice in Cedar Grove and West Milford, NJ. He can be reached at [email protected].
Dr. Lehrman was a periodontist with practices in New York City and Southampton, NY. Upon completion of his postgraduate training and his exposure to laser-assisted regenerative surgery in 2006, Dr. Lehrman dedicated his clinical practice to the treatment of periodontal, peri-implant, and cosmetic periodontic cases with a laser-assisted approach. He was engaged in both clinical and laboratory research with an eye toward creating “wound healing” with the advent of the Nd:YAG wavelength.
Dr. Annemarie O. Athansios obtained her DMD degree graduating with honors from RSDM. While at RSDM she was selected by the faculty committee for exceptional professionalism and ethics granting her the “Professionalism Award” and. In addition, she was also recognized for her volunteer work by the NJDA and was acknowledged with the “Give Kids a Smile Award”. Dr. Athansios received her postgraduate 3-year residency training in periodontics and earned her Masters of Dental Science degree at Rutgers university. During her post-graduate tenure, Dr. Athansios presented at Tri-school Symposium, served as chief resident, received a degree from the Institute of Advanced Laser Dentistry, and was awarded the Michael J. Deasy Endowed Scholarship. She mentors many students at the high school and college level that wish pursue a career in dentistry and enjoys going on mission trips with colleagues to renders dental treatment to the underprivileged communities in foreign countries such as Bolivia, Dominican Republic, and Egypt. She can be reached at [email protected].
Dr. Honigman is an assistant professor and head of LANAP training in the Department of Periodontics at RSDM. He holds bachelors degrees in biochemistry and genetics, and masters degrees in microbiology and immunology. He completed his doctorate degree from UTHSCSA and his degree in periodontics from UCLA. He is a certified instructor for the IALD and lectures nationally and internationally on LANAP and associated topics. He can be reached at [email protected].
Dr. Drew is a professor, director of implantology, and vice chairman in the Department of Periodontics at RSDM. He received his doctorate and degree in periodontics from RSDM. He has been awarded the RSDM Excellence in Teaching Award, Stuart D. Cook Master Educators Guild Award, and the prestigious American Academy of Periodontology Educator Award. Dr. Drew was inducted into the American College of Dentists, and he was awarded the RSDM Alumni Association Decade (1980s) Award. He has written for more than 35 publications and has lectured throughout the country. He was in full-time clinical practice for more than 25 years. He can be reached at [email protected].
Dr. Cappetta is PG director and an assistant professor in the Department of Periodontics at RSDM. He can be reached at [email protected].
Disclosure: Dr. Honigman is a consultant for IALD. All other authors report no disclosures.

