
Radiographs are limited in their ability to identify small carious lesions. Accurate identification and localization of carious lesions can be a real aid not only for early detection, but for enhanced patient care as well.
Noninvasive sensitive in vivo caries detection has been reported in the literature since 1998. The theory is that, by means of appropriate excitation sources and porphyrin fluorescence detectors, it should be possible to identify the products known to be associated with the bacteria that are associated with dental caries.1 However, can fluorescence spectroscopy differentiate between healthy and carious tooth structure? Emission spectra of all types of carious lesions were shifted towards longer wavelengths (red shift), when compared to the spectra of the corresponding sound enamel which fluoresces green. This red shift was reported to be highest for dark brown spot lesions and lowest for white spot lesions.2 At the 405-nm wavelength, the area of the fluorescence bands at 455 and 500 nm differ statistically for natural carious lesions and sound tissue.3 Differentiation then can be accomplished to determine what is affected and healthy tooth structure.
This has applications with regards to pit and fissure portions of the tooth but also may be applied to smooth surfaces. One study reported that light- and dark-discolored root surface caries showed distinct fluorescence emission bands between 600 and 700 nm that were not present in sound root surface areas. These bands were strongest for wavelengths between 390 and 420 nm. The spectra of root caries revealed maximum excitation at around 405 nm.4
Caries detection is especially challenging at the margins of existing restorations. Current technology (ie, DIAGNOdent [KaVo]) has not proven effective when examining tooth structure adjacent to restorative materials. These technologies rely on penetration of a laser into the tooth structure to detect demineralization. As restorative materials defract light, an accurate assessment cannot be at the restorations margins with the Diagnodent. Conversely, the Spectra system (Air Techniques) utilizes the fluorescence of the porphyrins associated with specific bacteria associated with dental caries, so identification at a restorations margin may provide more definitive identification of recurrent caries.
|


EARLY DETECTION IS KEY
Detecting the bacteria associated with caries can make a real difference in overall patient care. Early detection is often the key to effective caries management. Although the tooth may appear healthy on the surface, its real condition underneath the surface—especially true for fissure caries—is often hard to detect. Use of an explorer can lead to cavitation of early lesions preventing remineralization due to the surface disruption or may lead to an acceleration of the caries process when the weak enamel overlaying the demineralized area is physically broached by an instrument.
Enhanced caries detection, which supports minimally invasive treatment regimens, along with simplified case presentations, make Spectra an innovative, indispensable tool.
Spectra offers a different view to noninvasive caries detection, enabling reliable tooth-by-tooth detection of fissure caries and caries on smooth surfaces. While other devices use numeric indicators to signal the presence of decay, Spectra uses a color visual system with software analysis to provide a picture of the tooth with visual representation of where tooth structure is deteriorating. Spectra is a fluorescence-based caries detection system that has received FDA clearance. Spectra’s LEDs project high-energy blue light onto the tooth surface. Light of this wavelength stimulates bacteria to fluoresce red, whereas healthy enamel fluoresces green.
Flurorescence procedures are based on illustrating certain fluorescence substances like porphyrins, which grow in bacterial populated areas. When the area is stimulated with light of a certain wavelength, the molecules absorb the light energy and release part of the light energy with a different wavelength.
Spectra is similar to an intraoral camera in appearance and function. Yet, where an intraoral camera has white LEDs surrounding the lens, Spectra has an array of 6 LEDs emitting a 405 nm blue-violet light (Figure 1). Spectra connects to the operatory computer via a USB connector and is operated by proprietary software. The device is sheathed in a single-use disposable intraoral camera sleeve for sterility and an autoclavable rubber “spacer” is placed over the sheath at the end of the lens (Figure 2). The spacer eliminates ambient light and maintains a consistent distance between the device and the tooth surface, so images are reproducible and consistent. Spectra is both self-calibrating and portable, making it easy to use in offices with multiple operatories.
SPECTRA CARIES DETECTION PROTOCOL
The practitioner or hygienist, following removal of any plaque and tartar, which may interfere with caries detection, then utilizes the Spectra to capture pictures of the teeth. The spacer is placed over the dry tooth and kept in contact with the tooth to be analyzed, and then Spectra is activated to capture the image. When the image is frozen on the screen, either the Visix proprietary software (a special version of Visix is supplied with the Spectra system) or a twain driver (also available, allowing direct acquisition into most dental practice management software programs) analyzes the image, running an algorithm. Following instantaneous software analysis, the captured image on the computer of the tooth shows enamel breakdown due to caries in a graphic representation similar to weather radar images. Images can be saved to monitor areas or to gauge the effectiveness of remineralizing therapy.
It has long been recognized that the cariogenic bacteria Streptococcus mutans produces special metabolites called porphyrins. These porphyrins fluoresce when exposed to a 405-nm light. This fluorescence is detected by the Spectra device and is visually identified. The denser the bacterial colonization, the more intense the red fluorescent signal will be. The software analysis then provides the practitioner with an estimate of the depth and extent of the caries based on the color map produced, depending on the degree of fluorescence. These colors indicate the possible depth of carious involvement and help guide the practitioner to the appropriate treatment (Table). The image and corresponding color map also help in patient education and assist the patient in understanding why the avenue of treatment suggested is being recommended despite a possible absence of any tooth sensitivity.
 |
 |
|
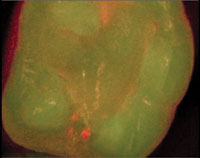
Figure 3. A healthy premolar image taken under detection mode with the Spectra unit. |
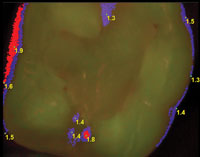
Figure 4. A healthy premolar image taken with the Spectra unit under analyze mode, showing no highlighted areas on the tooth surface. The red area shown is gingival tissue which may have bacteria containing porphyrins compounds. |
 |
 |
|
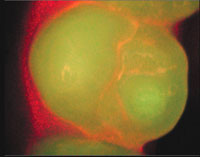
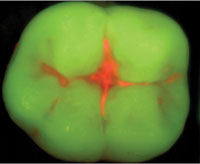
Figure 5. A premolar image taken with the Spectra unit under detection mode showing healthy tooth structure as green and questionable areas as red. |
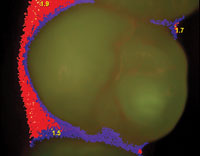
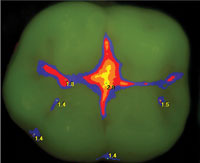
Figure 6. A premolar image taken with the Spectra unit under analyze mode demonstrating areas that may become carious in the future, allowing better patient education. |
 |
 |
|
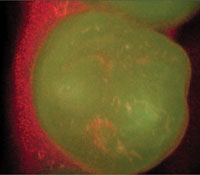
Figure 7. Molar captured with Spectra in detection mode showing suspect areas in the pits and fissures. |
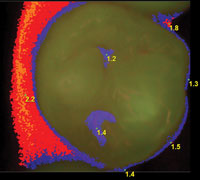
Figure 8. Molar captured with Spectra under analyze mode indicating a high value at the central pit. |
 |
 |
|
Figure 9. Preparation following removal of an existing composite restoration taken with Spectra. |
Figure 10. Preparation following removal of an existing composite restoration taken with Spectra under analyze mode, indicating decay still present in the mesial aspect of the preparation. |
The Spectra caries detection system provides the practitioner with a baseline for that patient’s particular tooth, allowing monitoring on subsequent recall appointments. Unlike competitive devices, the entire occlusal surface is analyzed and the image can be saved for future reference. Additionally, when remineralization procedures are employed, the practitioner can monitor how effective the remineralization proceeding.
| Table. Interpretation of Spectra (Air Techniques) data. |
 |
An added benefit to the Spectra device is in identifying bacteria-affected dentin during tooth preparation. Traditional methods, which include caries-indicating dye, have been reported to provide false positive or negative information which may lead to carious affected dentin being left or over excavation of healthy tooth structure. The fluorescence captured by the Spectra unit identifies porphyrins associated with S mutans and thus dentin in the preparation that fluoresces indicates the presence of bacteria in the dentin and can guide the practitioner to better decisions on caries excavation.
CASE EXAMPLES
Spectra can be utilized as a screening device at recall appointments. A healthy tooth may demonstrate slight fluorescence in the pits and fissures when observed under detection mode (Figure 3), but when switched to analyze mode, values should be zero in these areas (Figure 4). Whereas, a tooth with a similar appearance under detection mode (Figure 5) may, when switched to analyze mode, demonstrate some values in the pits and fissures (Figure 6). Low values in the pits and fissures may indicate continued observation of these areas or suggest either remineralization procedures be used or sealants placed. These images may also be used to educate the patient on areas of the tooth that require more home care attention. Teeth that show more extensive red fluorescence in the pits and fissures (Figure 7) may demonstrate higher values in these areas (Figure 8), leading the practitioner to perform conservative restorations versus observation until the caries have penetrated deeper and wider.
Another useful adjunct is in determining caries removal during preparation. A patient presented with a defective composite restoration in a mandibular molar. The Spectra unit was utilized following removal of the existing restoration to identify residual decay. Under detection mode, small areas of red fluorescence were noted (Figure 9). But, when switched to analyze mode, a higher value was noted in the mesiolingual aspect indicating that further excavation was needed at this spot (Figure 10).
High fluorescence associated with gingival tissue may be due to the presence of porphyrin-associated bacteria on the soft tissue. Some of the examples illustrated above demonstrate this. This can be used as an educational aid, directing the patient to areas that need better home care.
CONCLUSION
An innovative noninvasive caries detection system, Spectra shows the patient the presence of harmful bacteria in the mouth, and corresponding oral hygiene status. This can help motivate the patient to carry out a regimen of better dental care—both at home and through regular checkups and cleanings at the office.
Patient communication is important in our interactions when suggesting treatment. Frequently what is obvious to the practitioner, especially with regards to initial caries, is not clear to the patient. Patients usually base their decision process on initial fillings on sensitivity in the tooth and their trust in the practitioner. But when a tooth is not sensitive, it can be difficult to get the patient to move forward with early treatment. The Spectra system is another tool in our armamentarium aiding us in both diagnosis and communication with regards to incipient pit and fissure caries at the early stages. As an image is captured and values are set for specific areas of the occlusal of the posterior teeth, monitoring progress of the area when observation is decided versus clinical treatment. This allows patients to be a partner in their dental treatment and better understand the options of treatment or observation.
Additional information
For additional information, contact Air Techniques by calling (800) AIR-TECH or visit airtechniques.com.
References
- König K, Flemming G, Hibst R. Laser-induced autofluorescence spectroscopy of dental caries. Cell Mol Biol (Noisy-le-grand). 1998;44:1293-1300.
- Buchalla W. Compa
rative fluorescence spectroscopy shows differences in noncavitated enamel lesions. Caries Res. 2005;39:150-156. - Zezell DM, Ribeiro AC, Bachmann L, et al. Characterization of natural carious lesions by fluorescence spectroscopy at 405-nm excitation wavelength. J Biomed Opt. 2007;12:064013.
- Buchalla W, Lennon AM, Attin T. Comparative fluorescence spectroscopy of root caries lesions. Eur J Oral Sci. 2004;112:490-496.
Dr. Kurtzman is in private general practice in Silver Spring, Md, and is a former assistant clinical professor at the University of Maryland, department of endodontics, prosthetics and operative dentistry. A former assistant program director for a university-based implant maxi-course, he has earned Fellowship in the AGD, American College of Dentists, International Congress of Oral Implantologists (ICOI), Pierre Fauchard in the American College of Dentistry, Academy of Dentistry International, Mastership in the AGD and ICOI and Diplomat status in the ICOI and ADIA. He has lectured internationally on the topics of restorative dentistry, endodontics and implant surgery and prosthetics, removable and fixed prosthetics, periodontics, and has more than 180 published articles. He is privileged to be on the editorial board of numerous dental publications and is a consultant for multiple dental companies. He can be reached via e-mail at [email protected].
Disclosure: Dr. Kurtzman reports no disclosures.

