
INTRODUCTION
Patients presenting with functional and aesthetic concerns can be restored in a number of ways. Conventional treatment includes crown and bridgework, root canal therapy, core buildups, and removable partial dentures. With the advancement in implant dentistry, and the access to dental education for our patients through the Internet, dental implants have become an excellent alternative to our conventional procedures.
We all want the dentistry that we deliver to have an excellent long-term prognosis, especially when the care involves costly treatment plans. If a patient is investing thousands of dollars for an aesthetic and functional smile, neither patient nor dentist is pleased when things go wrong in a short period of time. This usually means that you will be “married” to this patient for a long time, redoing complicated dentistry that results in an unhappy patient and an even unhappier dentist. Before embarking on the dental implant journey with patients, it is important for every clinician to accomplish proper examinations and diagnostics to insure the highest rate of treatment success for a good long-term prognosis.
Evaluating Bruxism
One of the most important areas in which clinicians fail to do a proper evaluation is when care involves the treatment of bruxism. With one out of 3 patients having some level of bruxism, it is vitally important to get this under control with proper recognition and bruxism treatment before placing any implants or for that matter any dentistry.
There are 2 ways to evaluate a patient for destructive bruxism. One way is the physical examination of the patient. Most dentists are trained to detect the signs of tooth wear that are symptoms of bruxism. What we would like to focus on is what the American Academy of Facial Esthetics (AAFE) refers to as reading faces for bruxism and occlusal disease. You are probably wondering what a patient’s face has to do with bruxism in the mouth. In the experience of thousands of AAFE members who are dental professionals, we would all tell you that reading faces is much more important than seeing what is happening in the mouth.
Let’s look at a face together and it will be clear as to what the authors mean. Figure 1 shows the patient, who is the focus of the case report in this article, at rest. What do you see? If you learn to read her face, you will see very big masseter muscles with her left masseter being significantly larger than her right masseter. At rest, these muscles are unusually large, which means they are getting quite the workout to achieve that size. Indeed, they are the same as any other muscle in the body—the more you work it, the larger it gets. Would it surprise you that this patient has significant destructive bruxism? I don’t even have to look in her mouth to know it. She didn’t even have to tell me how the 8 bruxism appliances she had during the last few years—which she chewed through—didn’t help her at all. Most certainly, before we performed any restorative dentistry in her mouth, we would need to address these masseter muscles which provide all the power to her bruxism. This is what we refer to as reading faces.
If we want to confirm objectively how much bruxism this patient has, we can have her take an overnight bruxism/sleep monitor test (STATDDS). We in fact did administer this test and found that her bruxism episodes index (BEI) was 6.2, which gave us a baseline of the destructive bruxism that she had (a BEI greater than 5 is clinically destructive bruxism). It would be foolish to attempt any restorative dentistry, especially implant dentistry, without addressing her bruxism issues concretely. It is for this reason that Dr. Gordon Christensen1 has said, “Bruxism monitoring is one of the most important concepts in dentistry today.”
Using Botulinum Toxin in the Treatment of Bruxism
Botulinum toxin (Botox [Allergan] or Xeomin [STATDDS]) can be an excellent treatment option for bruxism. Botox reduces the intensity of contraction of the muscle through its mechanism of action of interrupting the neurotransmission of acetylcholine to the muscle. With proper training in the anatomy, physiology, pharmacology, and botulinum toxin delivery, a simple injection in each masseter would eliminate this patient’s bruxism and give her face a more aesthetic appearance. This was confirmed by a post-test with the STATDDS bruxism/sleep monitor, which now showed her BEI to be 0.6, effectively eliminating her bruxism. Even more so, this is clear by reading her face in the postoperative photo. In Figure 2, you can see for yourself that her bruxism is eliminated even without testing.
The advantages of using botulinum toxin for bruxism over any kind of appliance are that there are no compliance issues to deal with, and it is safe and effective. In this patient’s case, none of the bruxism appliances she had made were successful (she reported how each successive dentist told her the previous appliance wasn’t going to work, but the new one definitely would). Her bruxism and 12-year history of orofacial pain was completely resolved with a treatment plan consisting of botulinum toxin injections and trigger point therapy. It is important to let patients know that it takes botulinum toxin 2 to 10 days to begin to work after treatment and will last for 3 months, at which time the patient will need retreatment.
Once a patient’s bruxism is under control, then it is time to go inside the mouth, and implant treatment can begin and the clinician can feel confident of the long-term prognosis. Another way to deal with the results of bruxism is to use high-strength restorative materials that can withstand the impact of excessive bruxism.
CASE REPORT
Diagnosis and Treatment Planning
A 43-year-old female presented with a chief complaint of missing maxillary right and mandibular left dentition, broken-down bicuspid teeth, and unaesthetic and worn-down maxillary anterior teeth (Figures 3 to 5). Her maxillary right first bicuspid (tooth No. 5) was fractured, and she reported having pain in her second bicuspid (tooth No. 4) (Figure 6). She was unhappy with her smile and had several concerns, including pain in the upper right quadrant, fractured teeth, and loss of occlusion due to the missing maxillary right teeth and mandibular left teeth. It was determined that her mandibular teeth were in good repair and maintained aesthetic contours.
 |
 |
| Figure 1. Reading this patient’s face tells the clinician that she has been suffering from destructive bruxism and TMJ/orofacial pain. | Figure 2. After treatment with Botox (Allergan), her bruxism issues were resolved, allowing restorative treatment to begin. |
 |
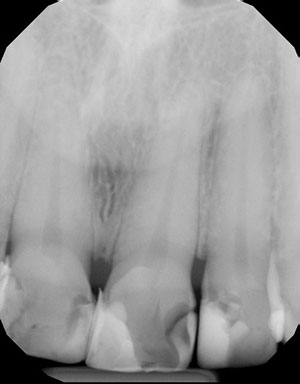 |
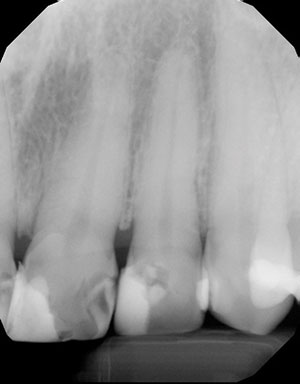
| Figure 3. This patient was a bruxer with worn maxillary teeth and some missing posterior teeth. | Figure 4. Digital periapical radiographs demonstrated large broken restorations along with caries. |
 |
 |
| Figure 5. This radiograph showed more of the same, including a significant loss of tooth structure on the cuspid due to bruxism. | Figure 6. Tooth No. 4 was deemed nonrestorable and endodontic therapy treatment was done on tooth No. 5. |
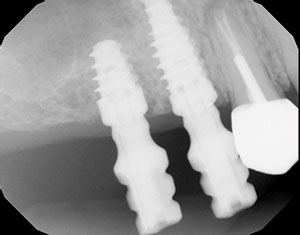
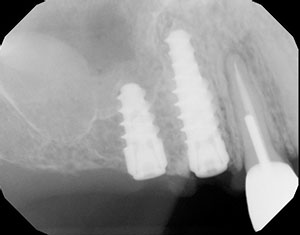 |
| Figure 7. Postoperative radiograph of the Hahn Tapered Implant System (Glidewell Laboratories) implants were ideally placed. |
When patients present with missing posterior occlusal stops, function then rests on the anterior teeth. This may result in excessive wear and un-aesthetic flattening of incisal edges due to her occlusion and bruxism.
She was also being treated for Crohn’s disease with Asacol and was previously diagnosed with micoadenoma pituitary gland.
We discussed the possibility of retaining teeth Nos. 4 and 5 and consulted with an endondontist who found tooth No. 4 unrestorable. A conventional post-and-core and crown would be completed on tooth No. 5.
The decision was made to restore the maxillary arch with implants and strong aesthetic crowns. This would increase the vertical dimension of occlusion, improve the length of the teeth to a younger appearance, and provide stability to the occlusion due to restoration of the posterior regions.
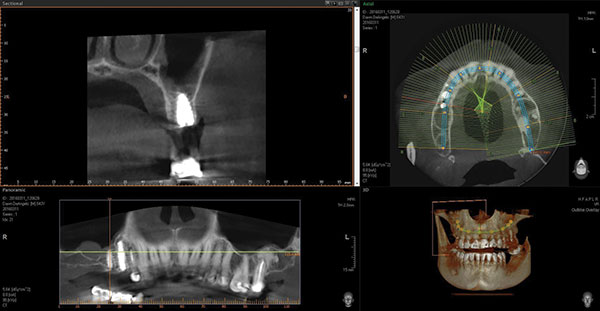 |
| Figure 8. Postoperative CBCT images (Vatech America) of implant in No. 3 position in proper orientation. |
 |
| Figure 9. Postoperative CBCT images (Vatech America) of implant in No. 4 position in proper orientation. |
Implant Treatment Protocol
For this case, the Hahn Tapered Implant System (Glidewell Laboratories) was to be used due to its innovative design and initial stability following surgical placement. The system allows the practitioner to angle and position the implant into available bone due to the pronounced threads that bore firmly to maximize bone adaptation. There is a buttress thread pattern that allows this stability and reduces bone resorption at the crest, which is often seen with other implant systems. Coronal microthreads help to preserve the crestal bone. The Hahn implant is processed with a resorbable blast media, which promotes osseointegration.2,3 There is also an intentional machined collar on the implant, which helps with soft-tissue health. The internal design of the implant is a conical hex connection. This connection ensures a firm and proper prosthetic seal. Note that the prosthetic design is one of platform switching, with all abutment connection on the inside of the body of the implant.
The surgical protocol for the Hahn Tapered Implant System is precise. First, a 2.2-mm diameter pilot drill is used to create the initial osteotomy. This establishes proper depth around any vital anatomy and the mesial-distal angulation of the implant. Dr. Kosinski prefers to parallel multiple implants to the natural tooth roots. Proper depth is determined radiographically. Next, 3.5-mm and 4.3-mm diameter osteotomy burs of established depth are used to create the final osteotomy. The Hahn implant is threaded into the prepared site and torque is established. Here, 40 Ncm of torque was achieved upon initial placement. Cover screws are inserted into the implants. The beveled surface of the implant is positioned slightly subcrestal in the immediate extraction socket, but at the crestal ridge of the edentulous molar site.
Using CAD/CAM designed and milled custom abutments allow for proper emergence profile and smile design. The margins are created at or just slightly subgingival to maintain tissue health and eliminate the possibility of cement staying in the gingival sulcus. Screw-retained crowns are used when the vertical occlusal space is compromised or where milled abutments would be too short to maintain a cement on crown. In this case, high translucency monolithic zirconia crowns would be used. This high-strength all-ceramic material is designed for long-term durability and yet to exhibit a more natural translucency than seen with the originally introduced zirconia materials. The implant-retained crowns are virtually designed and milled using the most innovative CAD/CAM technology.
 |
 |
| Figure 10. After a period of 4 months for osseointegration, the clinical work continued. Impression copings were placed into the internal design of the Hahn implants. | Figure 11. A radiograph was taken to ensure the complete seating of the impression copings. |
 |
 |
| Figure 12. The Glidewell Laboratories team fabricated an abutment for a screw-retained zirconia crown (BruxZir) for the No. 3 implant abutment. A custom abutment was fabricated for the No. 4 implant. | Figure 13. Occlusal view of the 2 implant crowns (Nos. 3 and 4) in place. |
 |
| Figure 13. Occlusal view of the 2 implant crowns (Nos. 3 and 4) in place. |
The treatment plan called for dental implants to be strategically placed in the maxillary right second bicuspid (No. 4 position) and first molar (No. 3 position) area, following atraumatic extraction of the nonrestorable second bicuspid tooth. The maxillary right first bicuspid (tooth No. 5) was treated with a post-and-core assembly and a new functional crown.
Clinical Treatment
Tooth No. 4 was atraumatically removed and the site grafted with Cerasorb Tri-Calcium Phosphate 250 to 1,000 μm (Curasan). Next, a 4.3-mm x 13-mm implant (Hahn Tapered Implant System) was immediately inserted and torqued to 40 Ncm. Then, a second 4.3-mm x 8-mm implant (Hahn Tapered Implant System) was also placed in the edentulous maxillary right first molar site using a flapless technique. The implant engaged bone anterior to the maxillary sinus (Figure 7). The implant placement was prepared and then verified for proper orientation and position with CBCT images (Vatech America) (Figures 8 and 9). Note that the immediate implant placement was about 1.0 mm subcrestal, allowing for proper physiologic reorganization of the bone.
The implants (Figures 10 and 11) were allowed to integrate for approximately 4 months prior to impressions and the fabrication of custom abutments and implant crowns.
The Glidewell Laboratories team fabricated a custom abutment for the maxillary right second bicuspid (No. 4) implant. Note that the margins were prepared at or just slightly subgingival to ensure that cement removal was simple and complete. A cement-retained zirconia crown (BruxZir [Glidewell Laboratories]) was placed (Improv [Salvin Dental Specialties]) on the No. 4 implant abutment. An abutment and screw-retained zirconia crown (BruxZir) for the No. 3 implant abutment was fabricated and placed. (The access opening would be easily concealed later using composite resin [Figures 11 to 13].)
The mandibular left posterior site was also restored with Hahn implants. The plane of occlusion was established using the mandibular arch, which was in better repair.
Due to the excessive wear of the maxillary anterior teeth, durable and aesthetic zirconia crowns (BruxZir Anterior [Glidewell Laboratories]) were prescribed and placed for teeth Nos. 6 to 12. This restorative choice gave the patient teeth with the desired aesthetics, while increasing the incisal opening to improve function and the patient’s overall facial aesthetics (Figure 14).
CLOSING COMMENTS
The days are over when a dentist simply gives a patient a bruxism appliance while thinking that the bruxism is adequately under control prior to any restorative and implant treatment. Clinicians have different options to deal with bruxism, and the treatment of this disease should be addressed before any restorative dentistry is accomplished. This article has presented the concepts and a case demonstrating the need for bruxism monitoring, treatment using Botox for the bruxism, and the use of high primary stability implants along with strong restorative materials.
Every dentist should seek and receive appropriate training in these diagnosis and treatment arenas. This will help clinicians ensure better therapeutic outcomes for their patients. Both of the authors are heavily involved with training general dentists in these areas, and every general dentist is capable of placing implants and using Botox treatment for bruxism. Get trained today!
References
- Malcmacher L, Christensen G. Botox and Dermal Fillers in Dentistry . Utah, Nev: PCC Dental; 2015.
- Piattelli M, Scarano A, Paolantonio M, et al. Bone response to machined and resorbable blast material titanium implants: an experimental study in rabbits. J Oral Implantol. 2002;28:2-8.
- Nishimoto SK, Nishimoto M, Park SW, et al. The effect of titanium surface roughening on protein absorption, cell attachment, and cell spreading. Int J Oral Maxillofac Implants. 2008;23:675-680.
Dr. Malcmacher is a practicing general dentist and an internationally known lecturer and author. He is the president of the American Academy of Facial Esthetics, and he can be reached at (800) 952-0521 or via email at [email protected].
Disclosure: Dr. Louis Malcmacher is an unpaid consultant for STATDDS.
Dr. Kosinski is an affiliate adjunct clinical professor at the University of Detroit Mercy School of Dentistry and is in private practice in Bingham Farms, Mich. He is currently the associate editor of the AGD journals. He is a Diplomate of the American Board of Oral Implantology/Implant Dentistry and the ICOI, and he is a Fellow of the AAID, ACD, ICD, and the ADI. He can be reached at [email protected].
Disclosure: Dr. Kosinski reports no disclosures.
Authors’ Note
Visit facialesthetics.org for information about live-patient Botox and dermal filler training, frontline TMJ/orofacial pain trigger point therapy, dental implant training, frontline dental sleep medicine, bruxism therapy and medical insurance, download Dr. Malcmacher’s resource list, and sign up for a free monthly e-newsletter.
Also By These Authors
The Dental Decision Maker: Reducing or Eliminating Failed Dentistry

