
Written by: Drs. Joseph Massad and Swati Ahuja
INTRODUCTION
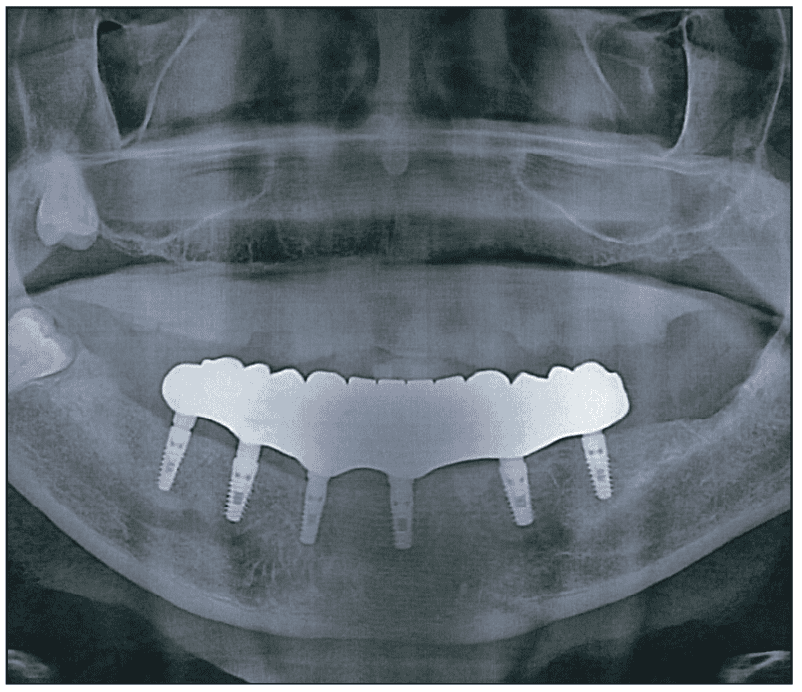
Fixed, full-arch, screw-retained implant prostheses (Figure 1) supported on titanium endosseous implants were first described in clinical studies conducted by a research group led by Per-Ingvar Brånemark.1,2 These early protocols involved placement of 4 to 6 endosseous implants in the anterior region of the mandible to support a fixed prosthesis.1,2 Long-term follow-up of this treatment concept, as reported by Brånemark and co-workers, demonstrated 10-year success rates ranging from 78.3% to 80.3% in the maxilla and 88.4% to 93.2% in the mandible.3 Currently, full-arch, fixed, implant-supported prostheses are a commonly prescribed treatment modality for the edentulous patient.4-6


Factors Affecting the Long-Term Success of Fixed Implant Restorations
The long-term success of fixed, full-arch restorations depends on several factors, including the availability of adequate restorative space, the prosthetic materials selected, and the mode of retention of the prosthesis.6-8
Restorative Space.Restorative space is the 3D oral space available to receive the proposed prosthodontic restoration (Figure 2).9 In edentulous patients, the available restorative space is bounded by the occlusal plane, supporting tissues of the edentulous jaw, facial tissues (cheeks and lips), and the tongue.9 Factors such as interocclusal rest space, phonetics, and aesthetics must also be considered when defining available restorative space.9 The minimum vertical restorative space required for fabricating a full-arch, fixed, screw-retained zirconia and a hybrid (metal-acrylic) restoration is 12 mm and 15 mm, respectively.8-10 Designing prostheses without considering the restorative space can result in restoration with inadequate contours, increased fracture susceptibility, and poor aesthetics.9 Insufficient restorative space may lead to the removal of existing non-restorable implants.11

Prosthetic Materials for Full-Arch Restorations.The material selected for fabricating an implant-supported restoration influences its success rate.12 Traditionally, metal-acrylic and metal-ceramic restorations were used, however, today, newer materials such as monolithic zirconia, ceramic-veneered zirconia, ceramic-veneered titanium, lithium disilicate, hybrid ceramics, milled PMMA (polymethyl methacrylate), PEEK (polyether ether ketone), and 3D-printed resins are now considered viable options for the fabrication of full-arch implant prostheses.12
Zirconia. Zirconia has become a preferred material for the fabrication of full-arch, implant-supported prostheses due to its superior aesthetics compared to metal-ceramic restorations, as well as its excellent mechanical properties and biocompatibility.12 Zirconia restorations have highly polished surfaces that promote favorable tissue contact and help maintain the health of the peri-implant tissues without causing adverse systemic reactions.12,13
Strengthening Zirconia With a Metal Framework.Zirconia is a ceramic, and like all ceramics, it is stronger in compression than in tension.14 Hence, it may be susceptible to fracture when used to support a long cantilever or when the forces are of greater magnitude and/or the restorative space is less than ideal. To enhance the durability and performance of zirconia restorations, incorporating a metal framework into the prosthesis design has proven to be an effective strategy (Figures 3a to 3d).15-18 However, when the joint between zirconia and metal is flat, the likelihood of fracture increases, particularly in high-stress areas. To address this issue, the metal structure may be designed to partly overlap the zirconia (Figure 3e), thereby reducing the risk of fracture and enhancing the restoration’s overall structural integrity.






Adhesive Cementation of Zirconia to Metal Framework.Achieving a reliable bond between zirconia and metal or titanium remains a significant challenge in prosthodontics. This protocol offers a step-by-step guide to help overcome these difficulties and ensure a stronger, more durable bond:
- Fit-check the anodized titanium framework and zirconia structure to eliminate overextensions and/or interferences. Next, finish, polish, clean, and air-dry the zirconia structure and the anodized titanium bar.
- Air-abrade the external surface of the anodized titanium framework, the internal surface of the zirconia structure, and the portion of the polished zirconia surface that will be overlapped by the metal using 50-µm aluminum oxide.19
- Apply a primer (Visalys Restorative Primer [Visalys]) to the air-abraded metal and zirconia surfaces, and air-dry after 60 seconds.19,20
- Use a dual-cure composite with Active Connect Technology (ACT) (Visalys CemCore [Visalys]) to coat the primed surfaces. Ensure bubble-free coverage.
- Carefully seat the metal framework onto the zirconia structure, and light-cure the entire assembly with a handheld unit till the elastic state is achieved. Eliminate the excess cement and then place the prosthesis in a light-curing unit for 5 minutes. Remove the prosthesis from the curing unit and thoroughly examine it for proper bonding (Figure 3f).
PMMA. Conventionally processed PMMA materials have several disadvantages, including increased polymerization shrinkage, susceptibility to microbial adhesion, radiolucency (lack of radio-opacity), potential for allergic reactions, and degradation of the mechanical properties of the material over time.21 The use of milled PMMA circumvents most of these disadvantages. CAD/CAM frameworks are more accurate compared to the casted frameworks developed by the lost wax technique.22 They have a passive fit, thereby decreasing the prosthesis movement and bacterial leakage.22
CAD/CAM frameworks may be milled or printed. Milled CAD/CAM frameworks are more accurate but significantly more expensive compared to printed CAD/CAM frameworks and conventional cast frameworks.23
Printed titanium frameworks (Figure 4a) are cost-effective and perform well clinically.23 Recently, full-arch implant restorations have been made using milled PMMA resin (Figure 4b) combined with a printed titanium frame (AvaMax hybrid prosthesis [AvaDent]) (Figure 4c).24 These prostheses are stronger because the PMMA resin is injected under high pressure (about 180 bar) as it bonds with the titanium frame.24 This method produces a more durable and affordable restoration compared with traditional metal-acrylic or zirconia options.24





The design features a digitally engineered titanium core shaped like a space truss, integrated into a dense acrylic base (Figures 4d and 4e).24 During injection, the PMMA flows through the titanium lattice, preventing separation between acrylic and metal, improving fracture resistance, and reducing flexibility compared with PMMA alone.24 A second design, known as the Montreal-style, uses the same injection process with a titanium truss framework that covers the entire tissue-side (intaglio) surface and slightly overlaps the outer PMMA on the buccal and lingual sides (Figures 4f to 4h).24 Both styles significantly improve strength and hardness compared with older designs.24



Retention Systems for Full-Arch Fixed Implant Restorations
The retention of fixed, full-arch, implant-supported restorations may involve screws, cement, abutments, or a combination of these systems.7,25,26 Choosing the appropriate retention system is challenging and affects the long-term success and survival of the restorations.7,21,22 Retrievability is an important factor to consider when choosing the type of retention.7
The full-arch, screw-retained hybrid prosthesis is retrievable, thereby permitting easier management of mechanical as well as biological complications after the placement of the restoration and during the maintenance phase.7,21,22 Screw-retained restorations require less vertical restorative space compared to cement-retained restorations.8 Since there is no cement used, there is no fear of leaving cement material, which may affect the health of the peri-implant tissues.7,25,26
However, there are a few disadvantages associated with screw-retained restorations. The fabrication of screw-retained prostheses is time-consuming as it requires several complex clinical and laboratory steps.7,25,26 Screw retention from the bone-level platform may make it difficult to fabricate a passive restoration, thereby necessitating the use of multi-unit abutments which are quite expensive.26 Thus, the overall cost of rendering this treatment is high. At the time of placement/removal of these restorations, small screws must be placed/removed from the mouth and if they accidentally fall into the oral cavity, there may be a possibility of aspiration. There may be accessibility issues, especially in the posterior quadrants of the mouth in patients with a limited oral opening.25 Screw-retained restorations are susceptible to screw loosening, screw fracture, fracture of prosthetic material around the screw access holes (as the screw channel compromises the stiffness of the material), and loss of covering material in the screw access holes. Achieving a truly passive fit in screw-retained restorations remains a challenge.7,25,27
An Abutment-Based Retentive System for Fixed Implant-Supported Prostheses
The LOCATOR FIXED Attachment System (Zest Dental Solutions) (Figure 5a) permits the fabrication of a retrievable fixed restoration that can be easily removed by the dental practitioner for maintenance of hygiene or performance of repairs.28


The same legacy LOCATOR abutments that are used for retaining removable implant prostheses are utilized to support and retain fixed implant prostheses by simply switching the conventional LOCATOR housings and inserts with LOCATOR FIXED housings (that provide superior and rigid engagement) and PEEK inserts (Figure 5b). It is a simple yet rigid abutment-based retentive system; it eliminates the need for cement, screw-access channels, retention screws, and composite filling materials.28 The LOCATOR FIXED attachment system now includes angled abutments. This innovation eliminates the need for the multi-unit abutments (MUAs), which simplifies the clinical procedure while reducing both cost and complexity.
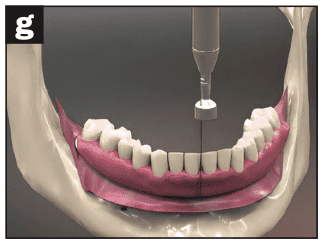
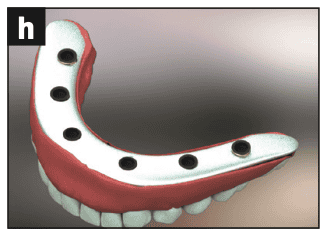
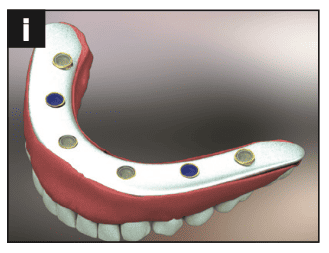
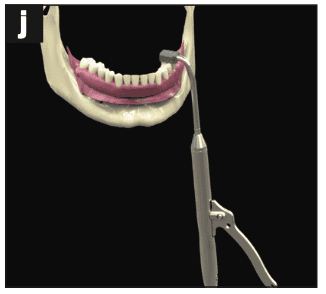
The procedural steps used to fabricate a fixed, full-arch prosthesis with the LOCATOR FIXED Attachment System are similar to those used to fabricate an implant overdenture supported by the conventional LOCATOR Attachment System.28 The retentive housings can be picked up in the prosthesis through a chairside procedure (similar to the LOCATOR Attachment System), thereby permitting the fabrication of a passive restoration (Figures 6 to 8).28 Because both the clinical steps and laboratory procedures are greatly simplified with this fixed attachment system, prostheses supported by the system can be fabricated and placed quickly and cost-effectively.28 Compared with screw-retained restorations, the placement and the removal of the LOCATOR FIXED restoration is less complicated and less time-consuming. As the restoration has no coping screws and no access channels to fill the problems such as screw loosening, screw fracture, material fracture adjacent to the screw axis holes, and loss of the screw access filling material are eliminated.28 This attachment system requires less vertical restorative space compared to other abutment-based retentive systems. Also, it provides a pleasing aesthetic result owing to the elimination of the screw access holes.28







With the Locator FIXED attachment system, a specialized tool is used for prosthetic removal. The use of this tool may exert pressure at critical points, which can create stress on the prosthesis. To minimize the risk of breakage at these stress points, it is recommended to use a metal bar that overlaps the zirconia/ceramic/PMMA in the prosthesis design. This overlap reinforces the restoration and enhances durability, especially in high-stress areas.
One of the key advantages of the LOCATOR FIXED Attachment System is its versatility. A seamless transition from removable implant prosthesis to fixed implant prosthesis and vice versa is possible by using the same abutment simply by switching out the inserts and housings in the existing prosthesis (followed by the fabrication of a new prosthesis later).28 The removable LOCATOR solution uses a flexible nylon insert and silver housing, and the FIXED offering uses proprietary rigid inserts and special gold housing.28 The LOCATOR FIXED Attachment System also permits staged treatment in patients with financial limitations. Initially, fewer implants can be placed and a removable prosthesis can be fabricated for the patient with the option of adding more implants in the future and converting the removable to a fixed implant prosthesis later. This system also permits a 20° correction per implant in any direction.28 It can be used for the fabrication of both transitional and definitive restorations.28
The new LOCATOR FIXED Attachment System is indicated for the rigid connection of partial (with cross-arch stabilization) and full-arch restorations on endosseous dental implants in the maxilla or mandible. It can be used to retain newly fabricated fixed restorations or to convert a patient’s existing full denture to a transitional fixed restoration.28 The LOCATOR FIXED attachment system offers an economical alternative to more complex and costly fixed implant prosthetic options.27 This system is simple yet predictable, and permits chairside pick-up of housings which results in decreased laboratory fees, number of appointments, and chair time.28 A minimum of 4 implants with adequate anterior-posterior spread (to minimize the cantilever length) is recommended for the fabrication of a full-arch, fixed restoration using the LOCATOR FIXED Attachment System. Also, it is recommended to use longer (>10 mm) and wide-diameter implants (>4 mm) in the posterior regions of the jaw to adequately support a full-arch “all on X” prostheses.
SUMMARY
The LOCATOR FIXED Attachment System significantly simplifies both clinical and laboratory procedures, enabling quick, cost-effective fabrication and placement of prostheses. While it is retrievable like screw-retained restorations, the placement and removal of the LOCATOR FIXED restoration are less complex and time-consuming. This system eliminates common issues such as screw loosening, screw fracture, material fractures near screw axis holes, and the need for filling screw access channels, as it has no coping screws or access holes. Additionally, the LOCATOR FIXED system requires less vertical restorative space than other abutment-based retentive systems and provides a more aesthetically pleasing result by eliminating screw access holes.
ACKNOWLEDGEMENTS
The authors would like to thank Chris Urist (primotec USA), Paul Kim (Dentcore), Johnny Orfinatas (Ameri-Dent Dental Laboratory), Jim Smyros and Joshua Rogers (AvaDent Digital Dental Solutions), and Daniel Parrilli (Kettenbach USA) for their lab support.
REFERENCES
1. Adell R, Lekholm U, Rockler B, et al. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg. 1981;10(6):387-416. doi:10.1016/s0300-9785(81)80077-4
2. Adell R, Eriksson B, Lekholm U, et al. Long-term follow-up study of osseointegrated implants in the treatment of totally edentulous jaws. Int J Oral Maxillofac Implants. 1990;5(4):347–59.
3. Brånemark PI, Svensson B, van Steenberghe D. Ten-year survival rates of fixed prostheses on four or six implants ad modum Brånemark in full edentulism. Clin Oral Implants Res. 1995;6(4):227–31. doi:10.1034/j.1600-0501.1995.060405.x
4. AlTarawneh S, Thalji G, Cooper L. Full-arch implant-supported monolithic zirconia fixed dental prostheses: An updated systematic review. Int J Oral Implantol (Berl). 2021;14(1):13-22.
5. Chan MH, Nudell YA. All-on-4 concept update. Dent Clin North Am. 2021;65(1):211–27. doi:10.1016/j.cden.2020.09.014
6. Cinquini C, Alfonsi F, Marchio V, et al. The use of zirconia for implant-supported fixed complete dental prostheses: a narrative review. Dent J (Basel). 2023;11(6):144. doi:10.3390/dj11060144
7. Gaddale R, Mishra SK, Chowdhary R. Complications of screw- and cement-retained implant-supported full-arch restorations: a systematic review and meta-analysis. Int J Oral Implantol (Berl). 2020;13(1):11-40.
8. Carpentieri J, Greenstein G, Cavallaro J. Hierarchy of restorative space required for different types of dental implant prostheses. J Am Dent Assoc. 2019;150(8):695-706. doi:10.1016/j.adaj.2019.04.015
9. Ahuja S, Cagna DR. Defining available restorative space for implant overdentures. J Prosthet Dent. 2010;104(2):133–6. doi:10.1016/S0022-3913(10)60107-2
10. Tischler M, Patch C, Bidra AS. Rehabilitation of edentulous jaws with zirconia complete-arch fixed implant-supported prostheses: An up to 4-year retrospective clinical study. J Prosthet Dent. 2018;120(2):204–9. doi:10.1016/j.prosdent.2017.12.010
11. Alhashim A, Harris RL, Zaher A, et al. Full-mouth rehabilitation with fixed, implant-supported prostheses. Inside Dentistry. 2012;17(12):18.
12. Ionescu RN, Totan AR, Imre MM, et al. Prosthetic materials used for implant-supported restorations and their biochemical oral interactions: a narrative review. Materials (Basel). 2022;15(3):1016. doi:10.3390/ma15031016
13. Gautam C, Joyner J, Gautam A, et al. Zirconia-based dental ceramics: structure, mechanical properties, biocompatibility, and applications. Dalton Trans. 2016;45(48):19194–215. doi:10.1039/c6dt03484e
14. Han J, Zhao J, Shen Z. Zirconia ceramics in metal-free implant dentistry. Adv Appl Ceram. 2017;116(3):138-150. doi:10.1080/17436753.2016.1264537
15. Drago C, Howell K. Concepts for designing and fabricating metal implant frameworks for hybrid implant prostheses. J Prosthodont. 2012;21(5):413–24. doi:10.1111/j.1532-849X.2012.00835.x
16. Ahuja S, Jain V, Cagna D, et al. Fabricating a mandibular implant-supported overdenture with a suspended framework. J Indian Prosthodont Soc. 2013;13(2):132–6. doi:10.1007/s13191-012-0196-8
17. Parpaiola A, Toia M, Norton M, et al. Fully digital workflow for implant-supported fixed restorations consisting of a titanium primary structure and a zirconia secondary structure. Int J Oral Implantol (Berl). 2023;16(4):351–8.
18. Pelekanos S, Ntovas P, Rizou V, et al. Translucent monolithic zirconia titanium-supported FP1 full-arch prosthesis: A novel proof of concept to address esthetic, functional, and biologic challenges. J Esthet Restor Dent. 2024;36(1):197-206. doi:10.1111/jerd.13167
19. Kitayama S, Nikaido T, Takahashi R, et al. Effect of primer treatment on bonding of resin cements to zirconia ceramic. Dent Mater. 2010;26(5):426–32. doi:10.1016/j.dental.2009.11.159
20. Koizumi H, Nakayama D, Komine F, et al. Bonding of resin-based luting cements to zirconia with and without the use of ceramic priming agents. J Adhes Dent. 2012;14(4):385–92. doi:10.3290/j.jad.a22711
21. Maeda Y, Minoura M, Tsutsumi S, et al. A CAD/CAM system for removable denture. Part I: Fabrication of complete dentures. Int J Prosthodont. 1994;7(1):17-21.
22. de Araújo GM, de França DG, Silva Neto JP, et al. Passivity of conventional and CAD/CAM fabricated implant frameworks. Braz Dent J. 2015;26(3):277–83. doi:10.1590/0103-6440201300145
23. Agarwal V, Nallaswamy D, V. Suresh, et al. Effectiveness of CAD-CAM milled versus DMLS titanium framework for hybrid denture prosthesis: a systematic review. J Pharm Neg Results. 2022;13(7):544–71. doi:10.47750/pnr.2022.13.S07.074
24. AvaDent. https://www.avadent.com. Accessed November 3, 2025.
25. Hamed MT, Abdullah Mously H, Khalid Alamoudi S, et al. A systematic review of screw versus cement-retained fixed implant-supported reconstructions. Clin Cosmet Investig Dent. 2020;12:9-16. doi:10.2147/ccide.s231070
26. Wittneben JG, Millen C, Brägger U. Clinical performance of screw- versus cement-retained fixed implant-supported reconstructions—a systematic review. Int J Oral Maxillofac Implants. 2014;29 Suppl:84-98. doi:10.11607/jomi.2014suppl.g2.1
27. Ashurko I, Trofimov A, Tarasenko S, et al. Full-mouth screw-retained implant-supported rehabilitation with multiunit abutments using virtual guided surgery and digital prosthetics protocol. Case Rep Dent. 2020;2020:3585169. doi:10.1155/2020/3585169
28. Zest Dental Solutions. https://www.zestdent.com. Accessed November 3, 2025.
ABOUT THE AUTHORS
Dr. Massad is an associate professor in the department of graduate prosthodontics at the University of Tennessee Health Science Center (UTHSC) College of Dentistry in Memphis; a clinical professor at the University of Oklahoma College of Dentistry in Oklahoma City; an associate faculty at the Tufts University School of Dental Medicine in Boston; an adjunct associate faculty of the department of comprehensive dentistry at the University of Texas Health Science Center at San Antonio (UT Health San Antonio) School of Dentistry; and an adjunct professor in the department of restorative dentistry at Loma Linda University in Loma Linda, Calif. He has a private practice in Tulsa. He can be reached at [email protected].
Dr. Ahuja is a former assistant professor in the department of prosthodontics at UTHSC in Memphis. She has lectured nationally and internationally on various prosthodontic topics at various dental conferences. She has been published in more than 50 peer-reviewed national and international journals and is also the co-author of the textbook Applications of the Neutral Zone in Prosthodontics. She is a consultant scientific writer and a consulting prosthodontist for several private dental clinics in Mumbai, India, and also for NYU Langone Medical Center in New York. She can be reached at [email protected].
Disclosures: Dr. Massad is a consultant for Zest Dental Solutions. He did not receive compensation for writing this article. Dr. Ahuja reports no disclosures.
FREE CE WEBINAR
Attachment Systems for Full-Arch Fixed Implant Restorations:
Materials, Space Requirements, and Retention Strategies
Presented by: Dr. Joseph Massad
VOD AVAILABLE NOW | CLICK HERE
AUDIO SUMMARY
Press play to listen to an audio summary from Dr. Joseph Massad.

