Written by: Gordon J. Christensen, DDS, MSD, PhD
INTRODUCTION
The dentistry of today doesn’t resemble the dentistry I was taught in dental school over one-half century ago. There has been an explosion of activity and many significant changes in clinical practice types, clinical procedures, practitioner gender, research, product development and sales, patient acceptance of procedures, and the overall direction of the profession.
Predicting what will happen in the future is a formidable task (Figure 1).
In my career, I have lived through and participated in almost all the following dental advancements:
- Local anesthetics introduced and welcomed
- Belt-driven handpieces to air rotor
- Hand tooth scaling to ultrasonic and hand scaling
- Silicate cement to resin-based composite materials
- Adhesive dentistry—acid etching and bonding, augmenting mechanical retention
- Many uses of fluoride for caries prevention, toothpastes, rinses, gels, etc.
- Amalgam’s reduction in use—alleged challenges still abound
- Development of impression materials to extremely accurate addition-reaction silicone
- Introduction of electric handpieces, bringing high torque and precision
- Cast gold alloy to porcelain-fused-to-metal, bringing improved aesthetics
- Metal-based restorations to ceramics with current continuing developments
- Various previously used implant designs to popular root-form implants
- In-office milling replacing most of metal casting
- The internet with major changes in all areas of life
- Digital radiography and cone beam
- Dental practice software
- Third-party payment
- DSOs
- Acceptance of titanium alloy implants over other previous implant materials
- Research showing ~50% of titanium alloy implants have peri-implantitis by ~10 yrs.
- Selective laser metal printing with improved accuracy and strength
- ~90% of indirect restorations ceramic – mostly zirconia
The above list doesn’t include the following technologies still in various stages of development (Figure 2):
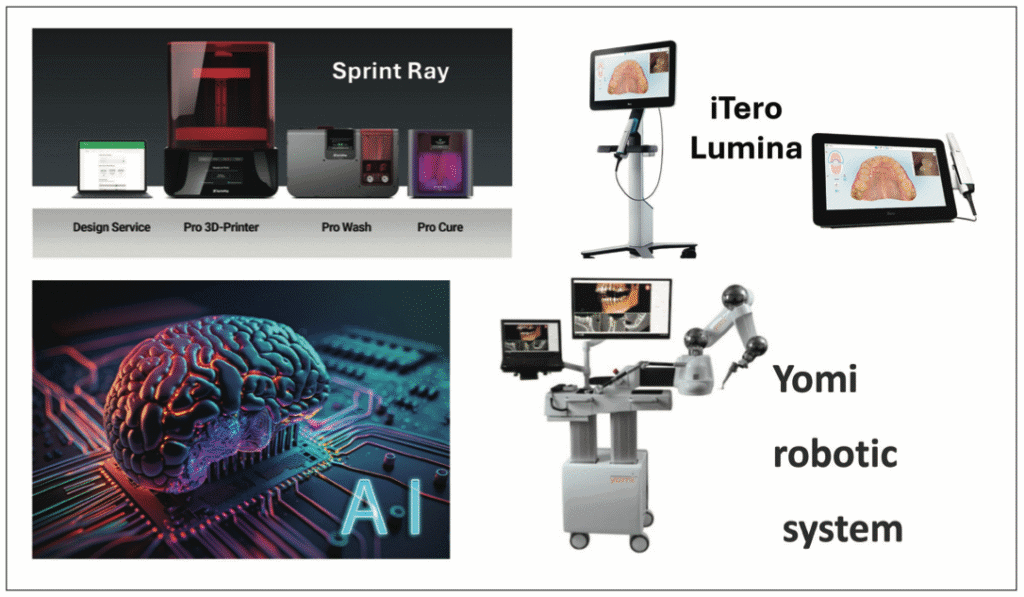
- Scanning, such as with iTero (Align Technology) is beginning to replace physical impressions with faster, easier use, and good patient acceptance, but higher cost
- Three-dimensional printing in labs and initiating in clinical use
- AI introduced and increasing in use
- Robotics , such as Yomi (Neocis), introduced and maturing for some situations
The previous concepts are an impressive list of developments. Some were eagerly and rapidly accepted, while others have only been slowly accepted over the past few years.
I have had many years evaluating thousands of dental concepts and products and watching their acceptance or rejection. The mantra for success we have recognized and accepted in Clinicians Report Foundation is: The concept, device, technology, material, or technique being introduced must be faster, easier, better, and less expensive than its predecessors to be successful.
The Status Quo of the Dental Profession
There are 202,300 dentists in America, including about 43,000 in 1 or more of the 12 recognized dental specialties—and public health officials have reported that we still need about 10,000 more dentists in the US to serve underserved areas.
In my considered opinion, depending on geographic location, some areas have far too many specialists and others have none, requiring patients to travel many miles to larger cities for treatment. Additionally, there are other areas of dentistry vying for specialty status by the ADA.
Dentistry in the US is providing adequate to excellent oral care to most of the population. Several organizations, including the ADA, estimate that about 65% to 70% of adults see a dentist at least once per year. But those estimates show we still have a significant percentage of potential patients who are not seeing dentists because of cost, fear, limited access to a dentist, or other reasons.
Areas in Dentistry Still Needing Research and Development
Although the status quo of US dentistry is impressive and unprecedented progress has been made over the last century, in my opinion, many areas of dentistry still need improvement. Why do I think these improvements have not been made to date? Research and development of new innovations is expensive, time-consuming, and fraught with regulations, paperwork, and strict academic requirements for research projects. Innovative dental manufacturers and academics usually conduct research, although some research-minded practitioners also contribute to developing new concepts.
I have compiled an example list of a few areas in dentistry that need immediate development and improvement. They are presented below in a nonprioritized list, with reasons for their needed changes and the positive changes I expect them to produce. I could provide many more examples!
Digital radiographic sensors that show initial caries and other details. Digital radiographic sensors have well-known positive characteristics, including storage capabilities, low radiation, lack of darkroom need, and other desirable features. I feel that compared to our experience with high-resolution radiographs film there are still some clinical inadequacies.
Current periapical and bite-wing radiographic sensors that use CMOS sensors or phosphor plate technology are strongly criticized by some practitioners. Which practitioners? Those who have used analog radiographic techniques and are familiar with older analog concepts that detect dental caries and small details more accurately than digital sensors. Dentists make hundreds of radiographs per month. Initial carious lesions and other small details blend into the many shades of gray in current digital sensors and are not visible to clinicians. New products using AI are helping to solve these challenges. Manufacturers are aware of these problems and they will be overcome.
In my opinion, manufacturers should take note. We need thin, flexible, inexpensive, easy-to-use digital sensors that show anatomic detail and pathologic conditions. For over 20 years, the profession has clamored for these characteristics, and there are massive opportunities if your product can fulfill our needs! (Figures 3 to 5.)

Cariostatic restorative materials. Except for glass ionomer, we do not have cariostatic restorative materials (Figure 6). Why do resin-based composite restorations look beautiful for a few months or years only and serve a fraction of the time that amalgam could? Composites are merely a plug in a hole cut in the tooth.

The margins are wide open, creating a happy place for microorganisms to live and reproduce. My current opinions on resin-based composites are:
- Many brands have similar characteristics.
- Most are using the same resin formulations with the same positive and negative characteristics seen in 1960.
- Most are available in putty, bulk, flowable, and reduced shades.
- Putty is well proven to be adequately cured in 2-mm increments. They have variable cure depth when more than 2.00 mm of cure is expected.
- Flowable resins have high interest. Some brands have nearly the same positive characteristics as putty, while others are less filled, resulting in excessive wear and shrinkage.
- Bulk-fill composites have mixed curing depths. Be careful. Some cure relatively well, others do not. Test them yourself.
- Reduced shades are a good concept for reducing inventory, though they come with some known limitations.
Continued challenges with resins include inadequate curing, often over-finishing with mutilated marginal white lines on completion, shrinkage of about 2%, relatively short longevity, lack of cariostatic properties, overall quality produced in clinical restorations could be better, and still need refinement of products.
In my opinion, we need a new, aesthetic, cariostatic, long-lasting, easily placed restorative material now!
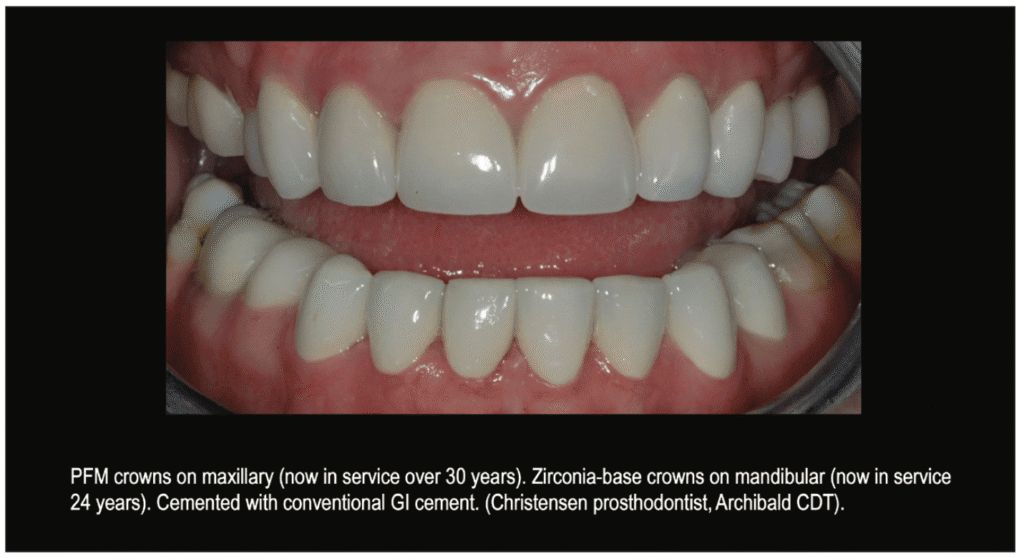
Cariostatic cement. All crowns, past and present, have always had open margins when analyzed by electron microscope. Current crowns have even more open margins due to computer-assisted spacing of digital dies, limitations of milling machines, and other challenges. Does it make sense to place a shrinking noncariostatic resin cement in those open margins? No! Resin-modified glass ionomers (RMGI) or conventional glass ionomers are the only current cements that can partially or fully overcome the caries-promoting problem. Recurrent caries at crown margins remains a significant and ongoing clinical problem (Figure 7).
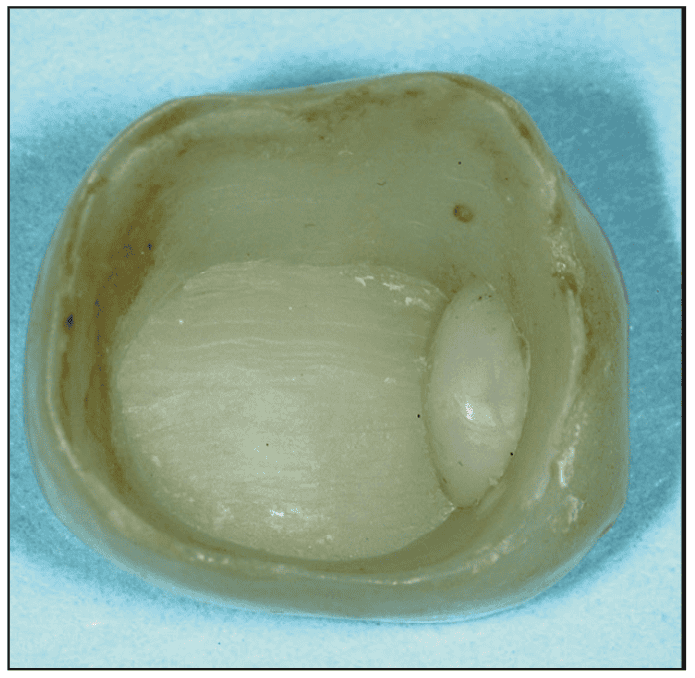
In my opinion, inventors and manufacturers, should please place emphasis on modifying or replacing current cariostatic cements to increase their cariostatic properties.
Scanners. These devices have been in dentistry since 1985 when CEREC was introduced. They have taken a long time to become popular. Why?8 High cost, significant learning curve, large size of scanners initially, and dentist satisfaction with inexpensive elastomer impressions. Currently, about 40% of practitioners use scanners instead of elastomers for impressions, as indicated by surveys and my observations of large CE groups.
I have some suggestions to make that percentage grow immediately. Can they reduce the size of scanners markedly to the size of a pencil? One advancement has been wireless technology that is more ergonomic. I am hoping that we can decrease the learning curve and create a size that can easily be placed into any mouth, small or large. Many have finally gotten rid of carts, keyboards, and any other inhibiting physical or infection control challenges. Some new manufacturers are significantly reducing prices.
I think this concept is too valuable to remain stagnant at its current level. Manufacturers: my call to action is that the first to introduce a new, inexpensive design will attract the entire dental market to adopt this desirable technology.
Three-dimensional printing. This technology is in the early adopter stage with clinicians and is primarily used clinically for objects with intermediate longevity needs. Study models, occlusal splints, sleep appliances, implant guides, etc, are the most used clinically produced objects. Will this concept make it to long-term restorative needs, such as crowns and fixed prostheses?
Manufacturers are pushing to create these resins as fully filled as possible. I surely hope so as many clinicians are still hesitant, and rightfully so. The technology is very new and we really don’t have long-term studies.
I will be pleased to see a low-wear resin crown developed specifically for implant-supported restorations to replace the rock-hard zirconia crowns now being placed on immovable implants, which are causing TMD and other clinical occlusal problems. The clinical and laboratory printing devices and techniques also need to be simplified and easy to understand. Progress is being made! An example is SprintRay has recently introduced a new concept—MIDAS, with higher filler content and strength.
Additionally, there is still confusion as to whether 3D printing is a clinical office or laboratory procedure, or both. Many dentists do not want to do laboratory work, and most who use 3D printing delegate the task to educated staff.
I believe that creative, innovative, realistic manufacturers can make this concept a viable clinical procedure for those interested. Whether or not it will become such for typical GPs is yet to be decided.
The preceding examples of needed changes are only a few of the current needs in dentistry. There are innumerable others I could easily tell any interested person or developer.
Current Factors Influencing Change in the Profession
There are many factors now influencing the future of dentistry. Here, I identify the factors I consider most important for preparing for the upcoming section on predictions that will impact the future of dentistry.
Artificial intelligence (AI). This factor is one of the most important, unpredictable, and yet-to-be-fully-trusted concepts. In recent surveys concerning AI by Clinicians Report Foundation, it was found the potential influence of AI is still relatively unknown to practicing dentists, yet it is being used in many forms by manufacturers to develop products, suggest techniques, and provide information to inventors, manufacturers, marketers, students, and essentially all the computer savvy public.
There is no question that AI will have a tremendous influence on the future of all aspects of life, including dentistry. Almost all the following factors will potentially be influenced by AI. It has high positive potential and significant unknown negative potential.
Education/training of dentists, staff, and patients. The introduction of AI has had wonderful effects and terrible repercussions to date. It has allowed students to write essays without thinking for themselves, which is frustrating educators at all levels. Conversely, although not yet refined or trusted, AI allows anyone to obtain information on any topic in seconds with a single click, but the user still has to be cognizant as to how reliable this information is. New computer programs to weed out the incorrect and unproven information AI provides are needed immediately.
Teledentistry. Access to professional dental care is nearly impossible in some geographic areas, and it can require lengthy, expensive travel. Consultation via teledentistry will certainly facilitate immediate diagnosis of some dental challenges, reduce costs, and improve patients’ access to information. It can also help monitor treatment progress without patients having to come back frequently. Its potential for dental treatment is being established, and its overall influence remains to be determined.
Personalized preventive and treatment procedures. The numerous specific factors related to the prevention and/or treatment of caries, periodontal disease, or occlusal challenges for a patient can and will be predicted and followed up on with help from AI. This concept has great potential for good, since in the past much of prevention and treatment was based on averages rather than the specific needs of individual patients.
Genomics. Genomics includes part of genetics. It concerns the characterization of all genes in an organism, rather than individual genes. The field uses a combination of laboratory and bioinformatic techniques to investigate the structure, function, evolution, and editing of genomes in specific patients. It has significant potential for preventive dentistry and for identifying which procedures are appropriate for a given patient’s specific needs.
Lasers. This technology has been available for my entire career, and there are hundreds of lasers of various wavelengths available for dental use. Overpromotion of the alleged advantages of lasers has slowed their growth in dentistry, but numerous surviving companies are realistic about the well-proven value of lasers in dentistry, and the concept continues to grow.
Robotics. One significant use of robotics—implant placement—has been refined significantly over the past decade and is assisting dentists well. Although expensive in its current form, robotics has the potential to be applied to many of the current human procedures.
Regenerative techniques. Regrowth or regeneration of tooth structure, bone, and soft tissue has great potential (Figures 9 to 10). Some concepts have already been proven and have led to the reformation of degenerated areas. Such current bioactive material examples have been proven to include:

- Bioactive glasses and ceramics. Materials promoting remineralization of enamel or dentin.
- Bioactive resin composites. Some hydrophilic composites release calcium, phosphate, or fluoride ions.
- Bioceramics in root canal sealers. Root canal sealers and other materials that promote healing and regeneration of the surrounding tissue.
Dentist physician interaction. As medicine evolved from the “barber-surgeon” times, dentistry was a significant part of overall medicine in the US. It is still a part of medicine in some countries. The designation of dentistry as a separate entity was started in 1840 with the establishment of the Baltimore College of Dental Surgery, and the DDS degree evolved. In my opinion, this was an unfortunate move and made dentists and physicians segregated to the disadvantage of their patients, since oral disease has now been shown to be connected to many systemic diseases.
AI has an opportunity to help reunite dentistry with the rest of medicine, especially by integrating the knowledge of both professions to assist one another and their respective patients.
DSOs in their various forms. These Dental Service Organizations (DSOs) have popularized both good and bad concepts within the profession. They provide a location for new graduates to build real-world knowledge and clinical skills and still have a respectable salary. The typical new grad going into a DSO stays from 1 to 3 years. Some mid-career dentists have also joined DSOs to lead a more normal lifestyle without the known stress of private practice. Estimates from the ADA and other sources indicate that mature dentists account for about 20% to 30% of the DSO population. DSOs have significantly improved practice efficiency and made other improvements.
However, as would be expected, there are some disadvantages of DSOs, including some that stress productivity and revenue over conservative patient care and patient interests.
The Potential Future of Dentistry
So far you have read about unbelievable advancements of the past several decades, pondered the frustrating and uncertain status quo of the profession and its needs, seen a few examples of the obvious need for research and development, and considered some of the factors now influencing the future. Now we will consider how all of these factors combined will influence dentistry and our practices in the future.
I see the following potential developments for the future:
- AI will continue to be an unknown, both helping and potentially hindering. It will be an increasingly important part of everything we do, not just in dentistry but in all aspects of life.
- Most aspects of dentistry will have a digital component, requiring dentists to understand the differences between digital and analog procedures and the advantages and limitations of each.
- Practices, both large and small, will be digitally connected to all areas of involvement, including dental labs, specialists, other general dentists, dental companies, distributors, patients, family, religion, and most other aspects of life.
- DSOs will continue to grow, providing both advantages and disadvantages for the profession, and most new graduates will use them as a stepping stone to whatever they want to do and become in the profession.
- Private practice, including group practices, will remain the mainstay of the profession, as many patients and practitioners prefer it.
- Technology will continue to grow. Technologies now in the early stages of development will either improve and become practical, clinically effective, cost-effective, and useful, or they will cease to be used.
- Preventive concepts will become far more important than they are now because of patient demand, and research funding and practical research in prevention will begin to replace the now-dominant financial emphasis ontherestoration of primarily edentulous patients.
- The new or currently still developing concepts as described in this article, including better sensors, cariostatic restorative materials, cariostatic cements, regenerative techniques, scanners, 3D printing, and myriad others will either prove themselves to be faster, easier, better, and less expensive than previous concepts or they will fade away.
- Some dentists will reject many of the new changes and continue to practice in the manner they prefer, which will still be adequate for several years.
- Other concepts yet to be invented or discovered will be identified and may even exceed in usefulness the many advancements of the past few decades.
SUMMARY
Dentistry is alive and well. It is a mandatory and essential health service. The causes of the 3 major diseases or conditions prevented or treated in dentistry—caries, periodontal disease, and occlusal diseases—will continue to be researched, and progress will be made toward curing them. However, the lack of patient compliance with known dental preventive procedures will undoubtedly continue to be a major need for overall dental services.
ABOUT THE AUTHOR
Dr. Christensen is founder and chief executive officer of Practical Clinical Courses (PCC), Senior Consultant & Previous CEO of Clinicians Report Foundation (CR), and a Practicing Prosthodontist in Provo, Utah. He is a co-founder of the non-profit CLINICIANS REPORT FOUNDATION (previously named CRA). Since 1976, the foundation has conducted research in all areas of dentistry and published the findings to the profession in the well-known CRA Newsletter now called CLINICIANS REPORT. Dr. Christensen’s degrees include: DDS from the University of Southern California; MSD from the University of Washington; PhD from the University of Denver; and 2 honorary doctorates. Early in his career, he helped establish the University of Kentucky and the University of Colorado dental schools, and taught at the University of Washington. Currently, he is an adjunct professor at the University of Utah School of Dentistry. He has presented thousands of hours of continuing education globally, produced hundreds of educational videos used worldwide, and published widely. He can be reached at (800) 223-6569 or [email protected].
Disclosure: Dr. Christensen reports no disclosures.
FREE CE WEBINAR
Dr. Gordon Christensen will present a FREE CE WEBINAR that will follow up on this article.